Volume 12, Issue 2 (10-2024)
Jorjani Biomed J 2024, 12(2): 10-13 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Omidi F, Fozouni L, Nikyar A, Mahmood Janlou M A. Sensitivity profile of carbapenem-resistant uropathogenic bacterial isolates to Cefiderocol. Jorjani Biomed J 2024; 12 (2) :10-13
URL: http://goums.ac.ir/jorjanijournal/article-1-1044-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-1044-en.html



1- Department of Microbiology, Gorgan Branch, Islamic Azad University, Gorgan, Iran
2- Department of Microbiology, Gorgan Branch, Islamic Azad University, Gorgan, Iran ,lili_kia@yahoo.com
3- Department of Research and Technology, Golestan Univeristy of Medical Sciences, Gorgan, Iran
4- Department of Biophysics, Faculty of Biological Sciences, Gorgan Branch, Islamic Azad University, Gorgan, Iran
2- Department of Microbiology, Gorgan Branch, Islamic Azad University, Gorgan, Iran ,
3- Department of Research and Technology, Golestan Univeristy of Medical Sciences, Gorgan, Iran
4- Department of Biophysics, Faculty of Biological Sciences, Gorgan Branch, Islamic Azad University, Gorgan, Iran
Full-Text [PDF 423 kb]
(718 Downloads)
| Abstract (HTML) (2151 Views)
Results
Of the 90 culture-positive urine samples, 63 (48.83%) were identified as E. coli and 27 (20.93%) were identified as K. pneumoniae. Most positive samples were taken from patients aged above 45 years under dialysis (61.6%). According to the MHT, 45 and 25 samples were positive for E. coli and K. pneumoniae, respectively. In the genotypic assay, 42 out of 59 E. coli isolates (71.19%) were carbapenemase positive, among which 20 isolates had the blaKPC gene (47.61%), 21 isolates (50%) had the blaNDM gene, 38 isolates had the blaOXA gene (90.47%), and 19 isolates had the blaIMP gene (45.23%). Moreover, 24 out of 25 K. pneumoniae isolates (96%) contained the blaKPC gene. Table 2 represents the MIC of Cefiderocol against the Carbapenem-resistant isolates in comparison to other antibiotics. In MIC determination, 55.24% of carbapenem-resistant E. coli isolates were inhibited with ≤0.5 μg/ml of Cefiderocol, while 4.76% of the strains were resistant to the highest MIC of Cefiderocol (MIC90=2 μg/ml). The drug could also effectively inhibit 51% of carbapenem-resistant K. pneumoniae isolates at concentrations ≤0.25 μg/ml, while only two strains (8.33%) showed resistance to the highest MIC of Cefiderocol (MIC90=2 μg/ml).
Discussion
The excessive use of antibiotics has been regarded as the principal cause of the emergence of resistant bacteria and the spread of resistant genes. Moreover, the rise of MDR hospital-acquired infections has become a serious global health problem. As mentioned previously, UTI is the most common hospital-acquired infection, which is usually caused by E. coli and Klebsiella spp. Despite the efficacy of carbapenem antibiotics against ESBL-producing bacteria, the emergence of resistant Gram-negative pathogens has resulted in major treatment difficulties, causing remarkable human and financial losses globally. Carbapenems are the most potent antibiotics among all clinically available beta-lactam antibiotics and are used as last resort drugs to treat infection caused by multidrug-resistant Gram-negative bacteria. Reports of phenotypic resistance to carbapenems vary across the world (8,9). In 2018, a study in Italy found that 70% of E. coli isolates from UTIs were resistant to carbapenems (15). Similar studies from India and Nepal reported the frequency of carbapenem-resistant E. coli isolates as 29.03% (16) and 28.6% (17), respectively. In the current study, the genotypic investigation of carbapenemase-producing strains indicated that 71.19% of E. coli isolates were positive for carbapenemase, which is higher than the rates reported in previous studies (4,14,15). In addition, almost all K. pneumoniae isolates (96%) were identified as carbapenemase-producing. In a study in Egypt, 33.6% of samples from patients with confirmed K. pneumoniae infections (UTI and pneumonia) were carbapenem-resistant, among which 61.9% and 92.8% were positive for carbapenemase activity in the MHT and genotypic investigation, respectively (18). Given the high rate of resistance to Colistin, Fluoroquinolones, and Cephalosporins among Gram-negative uropathogenic isolates (3), investigated the antibacterial effect of Cefiderocol on resistant clinical isolates, especially Carbapenem-resistant isolates. In vitro studies have demonstrated the effectiveness of this antibiotic against all high-priority Carbapenem-resistant Gram-negative bacteria (7,8).
In the present study, 4.76% of the E. coli and K. pneumoniae isolates were resistant to Cefiderocol respectively (MIC90=2 μg/ml). A recent study (2023) in Italy reported the rate of Cefiderocol-resistance as 12% in E. coli and 11% in K. pneumoniae clinical isolates (19) which is notably higher than the rates observed in the current study. Moreover, MIC90 of Cefiderocol against E. coli and in K. pneumoniae isolates was reported as 2 μg/mL, which is consistent with current findings. Notably, E. coli and K. pneumoniae, were susceptible to Cefiderocol, meaning it is a potential therapy for patients with UTI infection with few treatment options as a result of toxicity or resistance. In another study, the MIC90 of Cefiderocol was determined as 0.5 μg/L against Acinetobacter baumannii and Pseudomonas aeruginosa and 1 μg/L against K. pneumoniae and Enterobacter cloacae. In line with findings, the study reported the higher efficacy of Cefiderocol against carbapenem-resistant Gram-negative bacteria compared with other antibiotics (20). In another study, Cefiderocol was introduced as a highly effective antimicrobial against MDR Gram-negative pathogens that could inhibit almost all carbapenem-resistant Gram-negative isolates (~95%) producing the New Delhi metallo-beta-lactamase (NDM), OXA-23-like, and OXA-24-like genes at concentrations ≤4 mg/l (21).
Similar to the present study, a study in China reported the great inhibitory activity of Cefiderocol against carbapenem-resistant K. pneumoniae, P. aeruginosa, and Stenotrophomonas maltophilia. However, the study reported a relatively high rate (~37%) of Cefiderocol-resistance among A. baumannii isolates, all of which were positive for the blaOXA-23 and blaTEM genes (22). In the present study, on average 5 % of Cefiderocol-resistance isolates had blaOXA gene. So, an alarmingly high prevalence of antibiotic resistance among uropathogenic E. coli and K. pneumoniae isolates was detected, which could have serious health and financial complications. This finding might indicate the indiscriminate and overuse of antibiotics in the study population, which needs to be addressed by healthcare policymakers. The limitations of this study were the low number of isolates by infection source, potential biases, and generalizability to other populations.
Conclusion
Based on the results of the present study, Cefiderocol is effective against Carbapenem-resistant clinical isolates of E. coli and K. pneumoniae even at low concentrations. Therefore, it is recommended to investigate in vivo efficiency of this antibiotic for treating complicated UTIs caused by these Gram-negative bacteria.
Acknowledgement
The authors are grateful to all those who helped in this study as well as the staff of the Microbiology Laboratory at the Islamic Azad University, Gorgan branch, Iran.
Funding sources
This research has been accomplished with the support of Microbiology lab, I.A.U, Gorgan branch and it is extracted from the MSc thesis of Fatemeh Omidi.
Ethical statement
This study was performed under the Declaration of Helsinki for medical research involving human subjects and received approval from the Ethics Committee of Islamic Azad University, Chalus Branch, Iran (Ethical approval code: 1401.018).
Conflicts of interest
The authors declare no conflict of interest.
Author contributions
LF contributed to study concept and edited the final manuscript. FO performed laboratory examinations and interpreted the data. All authors read and approved the final manuscript.
Full-Text: (456 Views)
Introduction
Antimicrobial Resistance (AMR) is a major global health problem with enormous socioeconomic consequences. One of the most important causes of urinary tract infections (UTIs) is Enterobacteriaceae including Escherichia coli (E. coli) and Klebsiella spp. which have become a global health challenge as a nosocomial infection. β-Lactams antibiotics consisting of Penicillin, Cephalosporins, Monobactams, and Carbapenems have been the most commonly used group of antibiotics since their discovery. World Health Organization (WHO) has recognized Carbapenem-resistant Enterobacterales (CRE) as a significant threat to public health owing to its rate of infection, high mortality rates and widespread transmission potential. The recent global emergence of Carbapenem resistance, particularly among Gram-negative pathogens, has become a major therapeutic obstacle, accompanied by great human and financial loss (1,2). Although carbapenemase and extended-spectrum beta-lactamases (ESBLs) genes can be present in various species, they are abundantly found in Enterobacterales such as K. pneumoniae, E. coli, and Enterobacter spp. UTI caused by these pathogens is considered a serious threat to the health of people in society because the lack of timely diagnosis and treatment can cause severe complications such as urinary tract disorders, scarring in the kidney parenchyma, high blood pressure, uremia and in pregnant women, it can lead to premature birth and even abortion (3). The mechanisms of resistance to carbapenems comprise the production of carbapenemase enzymes, increased activity of efflux pumps, increased production of AmpC beta-lactamases, and mutations in the porins within the outer membrane, which results in decreased outer membrane permeability among Gram-negative bacteria through mobile genetic elements and the transfer of resistance genes (4). The production of carbapenemase is the pivotal mechanism of resistance to this class of antibiotics, which can rapidly evolve among Gram-negative bacteria through mobile genetic elements and the transfer of resistance genes. According to the Ambler classification method, carbapenem-hydrolyzing enzymes are classified into four categories (A, B, C, and D) depending on their amino acid sequence. Class A carbapenemases are serine β-lactamases that have serine in their active site. Class A, B, and D carbapenemases have very similar amino acid sequences (5,6).
Given the magnitude of infections caused by multidrug-resistant bacteria, a novel injectable siderophore cephalosporin called Cefiderocol (Fetroja) has been developed that is capable of traversing the periplasmic space and evading β-lactamase and other mechanisms of resistance in Gram-negative bacteria. This antibiotic has profound efficacy against various carbapenemases and β-lactamases producing isolates and therefore has been approved by the U.S. Food and Drug Administration for the treatment of complicated UTIs. According to studies, Cefiderocol is recommended for the treatment of complicated UTI, especially in patients who have not responded to other agents (7,8). The presence of pyrrolidine and carboxypropanoxymino groups in the side chains of Cefiderocol, which resembles the chemical structure of cefepime and ceftazidime, respectively, can improve antimicrobial efficacy and stability as well as outer-membrane diffusion (9). Considering the importance of continuous monitoring of AMR and the superior properties of Cefiderocol compared with Ceftazidime-Avibactam and Meropenem for the management of Carbapenem-resistant Enterobacteriaceae infections (10), the present study aimed to investigate the phenotypic and genotypic susceptibility profiles of Cefiderocol in Carbapenem-resistant uropathogenic K. pneumoniae and E. coli isolates.
Methods
Study population
This study was performed by collecting non-duplicate urine samples from 129 dialysis patients (n=70) and kidney transplant recipients (n=59) from Feb. 2021 to Dec. 2022. The samples were selected randomly using the convenience sampling method. The sample size was determined at a confidence level of 95% using the following formula, where P1 is the number of urines collected from urology ward and P2 represents the number of urines with a positive carbapenemase production test:
.PNG)
The average age of the patients was 41.04 ± 11.02 years. Inclusion criteria were first referral to these medical centers and hospitalization for more than 72h with urinary symptoms including dysuria, frequency, and urgency. The specimens were taken from a first-morning urine drainage bag and then cultured on blood agar and MacConkey agar (Oxoid Ltd., UK). After incubation aerobically at 37 °C for 18–24 hours, bacterial identification was carried out to the species level using standard biochemical techniques. All isolates were confirmed using the automated VITEK system (bioMérieux, Marcyl'Étoile, France) (2,11).
Detection of carbapenemase-producing strains
Non-susceptibility (Resistance and semi-susceptibility) to one or more members of the carbapenem family or resistance to one or more of the third-generation Cephalosporins, including Cefotaxime and Ceftazidime were considered for the initial identification of carbapenemase-producing strains isolates (12). Carbapenemase production in the identified isolates (n=90), was examined by performing a modified Hodge test (MHT) (13). In brief, E. coli ATCC 25922 as a positive control was first used and then diluted 1:10 using physiological saline. Ertapenem disc (10 μg) was placed on the surface of Mueller Hinton Agar and the plate was incubated at 37 °C for 24 hours. Carbapenemase-producing strains were identified by observing a non-inhibition zone around the disk.
To confirm resistance to Carbapenems, the minimum inhibitory concentration (MIC) against Meropenem and Imipenem was determined using the Epsilometer test (Etest). According to the manufacturer’s instructions (E-test), a concentration of 0.5 McFarland turbidity was prepared from the isolates that were resistant to one of the carbapenem disks and cultured on Mueller Hinton agar. After a few minutes, two Etest strips of Imipenem and Meropenem were placed on the plates, which were then incubated at 37 °C for 24 hours. In the confirmatory test, K. pneumoniae ATCC 700603 and K. pneumoniae ATCC 1706 were used as the positive and negative control, respectively.
Genotypic detection of carbapenemase-producing strains
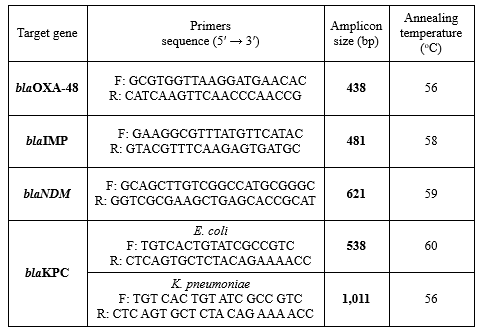
DNA extraction was performed using the boiling method (14). For this purpose, a suspension from the 24-hour bacterial cultures was prepared in sterile distilled water. Then, the supernatant was discarded and 100 µl of NaOH was added to the sediment. The tube was placed in a water bath at 95 °C. Finally, 20 mM Tris-HCl Buffer was added and the tube was centrifuged at 14,000 rpm. The obtained DNA-containing supernatant was separated and kept in a sterile Eppendorf tube collected, and stored at -20 °C. PCR was carried out for the detection of blaKPC, blaNDM, blaIMP, and blaOXA-48 genes among E. coli and K. pneumoniae isolates using specific primers (Table 1). The 25 μL PCR reactions contained 1μL of the DNA sample, 1 μL of each forward and reverse primers, 0.5 μL of dNTPs, 2.5 μL of PCR buffer (Sigma-Aldrich, USA), 0.75 μL of magnesium chloride, 1U of Taq polymerase enzyme and 18.05 μL of distilled water. Amplification was programmed for an initial denaturation at 94 °C for 5 min, followed by 35 cycles of denaturation at 95 °C for 30 sec, annealing at 55-60 °C for 30 sec, extension at 72 °C for 30 sec, and a final extension at 72 °C for 5 min. The PCR products were electrophoresed on 1.5% agarose gel (Sigma, USA), and the bands were visualized under UV light after staining with ethidium bromide.
Determination of MIC
The MIC of Cefotaxime, Imipenem, Cefiderocol, Meropenem, Cefepime, Ceftazidime/Avibactam, Ceftolozane/Tazobactam, Aztreonam, Amikacin, Levofloxacin, Colistin and Tigecycline against the isolates was determined by the standard broth microdilution assay using Mueller Hinton II Broth according to the recommendations of the CLSI-2021 (12). To prepare, the initial concentration of each antibiotic was inoculated into wells of a 96-well microplate containing Mueller Hinton broth (Merck, Germany). After preparing serial dilutions and inoculation of the bacterial suspension at a final concentration of 1.5 × 105 colony-forming units, the microplate was incubated at 37 °C for 20-24 hours. In addition, the MIC of Cefiderocol in iron-depleted cation-adjusted Mueller-Hinton broth (ID-CAMHB) was determined according to CLSI. The MIC of Cefiderocol was defined as the lowest concentration of the antibiotic that completely inhibited the growth of bacteria or the lowest concentration that significantly reduced the growth of bacteria compared to the control well. Results were interpreted as follows: MIC ≤4 μg/L was considered susceptible, 8 μg/L as intermediate, and ≥16 μg/L as resistant (12).
Antimicrobial Resistance (AMR) is a major global health problem with enormous socioeconomic consequences. One of the most important causes of urinary tract infections (UTIs) is Enterobacteriaceae including Escherichia coli (E. coli) and Klebsiella spp. which have become a global health challenge as a nosocomial infection. β-Lactams antibiotics consisting of Penicillin, Cephalosporins, Monobactams, and Carbapenems have been the most commonly used group of antibiotics since their discovery. World Health Organization (WHO) has recognized Carbapenem-resistant Enterobacterales (CRE) as a significant threat to public health owing to its rate of infection, high mortality rates and widespread transmission potential. The recent global emergence of Carbapenem resistance, particularly among Gram-negative pathogens, has become a major therapeutic obstacle, accompanied by great human and financial loss (1,2). Although carbapenemase and extended-spectrum beta-lactamases (ESBLs) genes can be present in various species, they are abundantly found in Enterobacterales such as K. pneumoniae, E. coli, and Enterobacter spp. UTI caused by these pathogens is considered a serious threat to the health of people in society because the lack of timely diagnosis and treatment can cause severe complications such as urinary tract disorders, scarring in the kidney parenchyma, high blood pressure, uremia and in pregnant women, it can lead to premature birth and even abortion (3). The mechanisms of resistance to carbapenems comprise the production of carbapenemase enzymes, increased activity of efflux pumps, increased production of AmpC beta-lactamases, and mutations in the porins within the outer membrane, which results in decreased outer membrane permeability among Gram-negative bacteria through mobile genetic elements and the transfer of resistance genes (4). The production of carbapenemase is the pivotal mechanism of resistance to this class of antibiotics, which can rapidly evolve among Gram-negative bacteria through mobile genetic elements and the transfer of resistance genes. According to the Ambler classification method, carbapenem-hydrolyzing enzymes are classified into four categories (A, B, C, and D) depending on their amino acid sequence. Class A carbapenemases are serine β-lactamases that have serine in their active site. Class A, B, and D carbapenemases have very similar amino acid sequences (5,6).
Given the magnitude of infections caused by multidrug-resistant bacteria, a novel injectable siderophore cephalosporin called Cefiderocol (Fetroja) has been developed that is capable of traversing the periplasmic space and evading β-lactamase and other mechanisms of resistance in Gram-negative bacteria. This antibiotic has profound efficacy against various carbapenemases and β-lactamases producing isolates and therefore has been approved by the U.S. Food and Drug Administration for the treatment of complicated UTIs. According to studies, Cefiderocol is recommended for the treatment of complicated UTI, especially in patients who have not responded to other agents (7,8). The presence of pyrrolidine and carboxypropanoxymino groups in the side chains of Cefiderocol, which resembles the chemical structure of cefepime and ceftazidime, respectively, can improve antimicrobial efficacy and stability as well as outer-membrane diffusion (9). Considering the importance of continuous monitoring of AMR and the superior properties of Cefiderocol compared with Ceftazidime-Avibactam and Meropenem for the management of Carbapenem-resistant Enterobacteriaceae infections (10), the present study aimed to investigate the phenotypic and genotypic susceptibility profiles of Cefiderocol in Carbapenem-resistant uropathogenic K. pneumoniae and E. coli isolates.
Methods
Study population
This study was performed by collecting non-duplicate urine samples from 129 dialysis patients (n=70) and kidney transplant recipients (n=59) from Feb. 2021 to Dec. 2022. The samples were selected randomly using the convenience sampling method. The sample size was determined at a confidence level of 95% using the following formula, where P1 is the number of urines collected from urology ward and P2 represents the number of urines with a positive carbapenemase production test:
The average age of the patients was 41.04 ± 11.02 years. Inclusion criteria were first referral to these medical centers and hospitalization for more than 72h with urinary symptoms including dysuria, frequency, and urgency. The specimens were taken from a first-morning urine drainage bag and then cultured on blood agar and MacConkey agar (Oxoid Ltd., UK). After incubation aerobically at 37 °C for 18–24 hours, bacterial identification was carried out to the species level using standard biochemical techniques. All isolates were confirmed using the automated VITEK system (bioMérieux, Marcyl'Étoile, France) (2,11).
Detection of carbapenemase-producing strains
Non-susceptibility (Resistance and semi-susceptibility) to one or more members of the carbapenem family or resistance to one or more of the third-generation Cephalosporins, including Cefotaxime and Ceftazidime were considered for the initial identification of carbapenemase-producing strains isolates (12). Carbapenemase production in the identified isolates (n=90), was examined by performing a modified Hodge test (MHT) (13). In brief, E. coli ATCC 25922 as a positive control was first used and then diluted 1:10 using physiological saline. Ertapenem disc (10 μg) was placed on the surface of Mueller Hinton Agar and the plate was incubated at 37 °C for 24 hours. Carbapenemase-producing strains were identified by observing a non-inhibition zone around the disk.
To confirm resistance to Carbapenems, the minimum inhibitory concentration (MIC) against Meropenem and Imipenem was determined using the Epsilometer test (Etest). According to the manufacturer’s instructions (E-test), a concentration of 0.5 McFarland turbidity was prepared from the isolates that were resistant to one of the carbapenem disks and cultured on Mueller Hinton agar. After a few minutes, two Etest strips of Imipenem and Meropenem were placed on the plates, which were then incubated at 37 °C for 24 hours. In the confirmatory test, K. pneumoniae ATCC 700603 and K. pneumoniae ATCC 1706 were used as the positive and negative control, respectively.
Genotypic detection of carbapenemase-producing strains
DNA extraction was performed using the boiling method (14). For this purpose, a suspension from the 24-hour bacterial cultures was prepared in sterile distilled water. Then, the supernatant was discarded and 100 µl of NaOH was added to the sediment. The tube was placed in a water bath at 95 °C. Finally, 20 mM Tris-HCl Buffer was added and the tube was centrifuged at 14,000 rpm. The obtained DNA-containing supernatant was separated and kept in a sterile Eppendorf tube collected, and stored at -20 °C. PCR was carried out for the detection of blaKPC, blaNDM, blaIMP, and blaOXA-48 genes among E. coli and K. pneumoniae isolates using specific primers (Table 1). The 25 μL PCR reactions contained 1μL of the DNA sample, 1 μL of each forward and reverse primers, 0.5 μL of dNTPs, 2.5 μL of PCR buffer (Sigma-Aldrich, USA), 0.75 μL of magnesium chloride, 1U of Taq polymerase enzyme and 18.05 μL of distilled water. Amplification was programmed for an initial denaturation at 94 °C for 5 min, followed by 35 cycles of denaturation at 95 °C for 30 sec, annealing at 55-60 °C for 30 sec, extension at 72 °C for 30 sec, and a final extension at 72 °C for 5 min. The PCR products were electrophoresed on 1.5% agarose gel (Sigma, USA), and the bands were visualized under UV light after staining with ethidium bromide.
Determination of MIC
The MIC of Cefotaxime, Imipenem, Cefiderocol, Meropenem, Cefepime, Ceftazidime/Avibactam, Ceftolozane/Tazobactam, Aztreonam, Amikacin, Levofloxacin, Colistin and Tigecycline against the isolates was determined by the standard broth microdilution assay using Mueller Hinton II Broth according to the recommendations of the CLSI-2021 (12). To prepare, the initial concentration of each antibiotic was inoculated into wells of a 96-well microplate containing Mueller Hinton broth (Merck, Germany). After preparing serial dilutions and inoculation of the bacterial suspension at a final concentration of 1.5 × 105 colony-forming units, the microplate was incubated at 37 °C for 20-24 hours. In addition, the MIC of Cefiderocol in iron-depleted cation-adjusted Mueller-Hinton broth (ID-CAMHB) was determined according to CLSI. The MIC of Cefiderocol was defined as the lowest concentration of the antibiotic that completely inhibited the growth of bacteria or the lowest concentration that significantly reduced the growth of bacteria compared to the control well. Results were interpreted as follows: MIC ≤4 μg/L was considered susceptible, 8 μg/L as intermediate, and ≥16 μg/L as resistant (12).
Results
Of the 90 culture-positive urine samples, 63 (48.83%) were identified as E. coli and 27 (20.93%) were identified as K. pneumoniae. Most positive samples were taken from patients aged above 45 years under dialysis (61.6%). According to the MHT, 45 and 25 samples were positive for E. coli and K. pneumoniae, respectively. In the genotypic assay, 42 out of 59 E. coli isolates (71.19%) were carbapenemase positive, among which 20 isolates had the blaKPC gene (47.61%), 21 isolates (50%) had the blaNDM gene, 38 isolates had the blaOXA gene (90.47%), and 19 isolates had the blaIMP gene (45.23%). Moreover, 24 out of 25 K. pneumoniae isolates (96%) contained the blaKPC gene. Table 2 represents the MIC of Cefiderocol against the Carbapenem-resistant isolates in comparison to other antibiotics. In MIC determination, 55.24% of carbapenem-resistant E. coli isolates were inhibited with ≤0.5 μg/ml of Cefiderocol, while 4.76% of the strains were resistant to the highest MIC of Cefiderocol (MIC90=2 μg/ml). The drug could also effectively inhibit 51% of carbapenem-resistant K. pneumoniae isolates at concentrations ≤0.25 μg/ml, while only two strains (8.33%) showed resistance to the highest MIC of Cefiderocol (MIC90=2 μg/ml).
Table 2. In vitro inhibitory activities of Cefiderocol and other antibiotics against carbapenem-resistant clinical isolates of K. pneumoniae (n=24) Table 3. In vitro inhibitory activities of Cefiderocol and other antibiotics against carbapenem-resistant clinical isolates of E. coli (n=42) 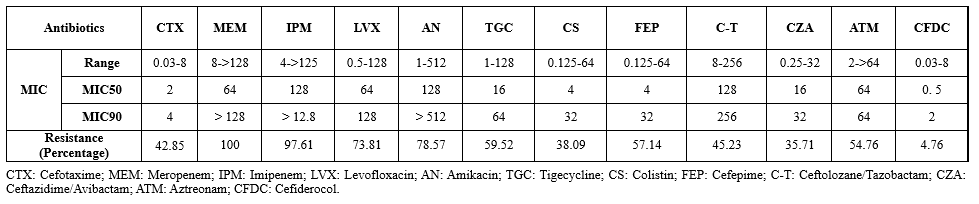 |
Discussion
The excessive use of antibiotics has been regarded as the principal cause of the emergence of resistant bacteria and the spread of resistant genes. Moreover, the rise of MDR hospital-acquired infections has become a serious global health problem. As mentioned previously, UTI is the most common hospital-acquired infection, which is usually caused by E. coli and Klebsiella spp. Despite the efficacy of carbapenem antibiotics against ESBL-producing bacteria, the emergence of resistant Gram-negative pathogens has resulted in major treatment difficulties, causing remarkable human and financial losses globally. Carbapenems are the most potent antibiotics among all clinically available beta-lactam antibiotics and are used as last resort drugs to treat infection caused by multidrug-resistant Gram-negative bacteria. Reports of phenotypic resistance to carbapenems vary across the world (8,9). In 2018, a study in Italy found that 70% of E. coli isolates from UTIs were resistant to carbapenems (15). Similar studies from India and Nepal reported the frequency of carbapenem-resistant E. coli isolates as 29.03% (16) and 28.6% (17), respectively. In the current study, the genotypic investigation of carbapenemase-producing strains indicated that 71.19% of E. coli isolates were positive for carbapenemase, which is higher than the rates reported in previous studies (4,14,15). In addition, almost all K. pneumoniae isolates (96%) were identified as carbapenemase-producing. In a study in Egypt, 33.6% of samples from patients with confirmed K. pneumoniae infections (UTI and pneumonia) were carbapenem-resistant, among which 61.9% and 92.8% were positive for carbapenemase activity in the MHT and genotypic investigation, respectively (18). Given the high rate of resistance to Colistin, Fluoroquinolones, and Cephalosporins among Gram-negative uropathogenic isolates (3), investigated the antibacterial effect of Cefiderocol on resistant clinical isolates, especially Carbapenem-resistant isolates. In vitro studies have demonstrated the effectiveness of this antibiotic against all high-priority Carbapenem-resistant Gram-negative bacteria (7,8).
In the present study, 4.76% of the E. coli and K. pneumoniae isolates were resistant to Cefiderocol respectively (MIC90=2 μg/ml). A recent study (2023) in Italy reported the rate of Cefiderocol-resistance as 12% in E. coli and 11% in K. pneumoniae clinical isolates (19) which is notably higher than the rates observed in the current study. Moreover, MIC90 of Cefiderocol against E. coli and in K. pneumoniae isolates was reported as 2 μg/mL, which is consistent with current findings. Notably, E. coli and K. pneumoniae, were susceptible to Cefiderocol, meaning it is a potential therapy for patients with UTI infection with few treatment options as a result of toxicity or resistance. In another study, the MIC90 of Cefiderocol was determined as 0.5 μg/L against Acinetobacter baumannii and Pseudomonas aeruginosa and 1 μg/L against K. pneumoniae and Enterobacter cloacae. In line with findings, the study reported the higher efficacy of Cefiderocol against carbapenem-resistant Gram-negative bacteria compared with other antibiotics (20). In another study, Cefiderocol was introduced as a highly effective antimicrobial against MDR Gram-negative pathogens that could inhibit almost all carbapenem-resistant Gram-negative isolates (~95%) producing the New Delhi metallo-beta-lactamase (NDM), OXA-23-like, and OXA-24-like genes at concentrations ≤4 mg/l (21).
Similar to the present study, a study in China reported the great inhibitory activity of Cefiderocol against carbapenem-resistant K. pneumoniae, P. aeruginosa, and Stenotrophomonas maltophilia. However, the study reported a relatively high rate (~37%) of Cefiderocol-resistance among A. baumannii isolates, all of which were positive for the blaOXA-23 and blaTEM genes (22). In the present study, on average 5 % of Cefiderocol-resistance isolates had blaOXA gene. So, an alarmingly high prevalence of antibiotic resistance among uropathogenic E. coli and K. pneumoniae isolates was detected, which could have serious health and financial complications. This finding might indicate the indiscriminate and overuse of antibiotics in the study population, which needs to be addressed by healthcare policymakers. The limitations of this study were the low number of isolates by infection source, potential biases, and generalizability to other populations.
Conclusion
Based on the results of the present study, Cefiderocol is effective against Carbapenem-resistant clinical isolates of E. coli and K. pneumoniae even at low concentrations. Therefore, it is recommended to investigate in vivo efficiency of this antibiotic for treating complicated UTIs caused by these Gram-negative bacteria.
Acknowledgement
The authors are grateful to all those who helped in this study as well as the staff of the Microbiology Laboratory at the Islamic Azad University, Gorgan branch, Iran.
Funding sources
This research has been accomplished with the support of Microbiology lab, I.A.U, Gorgan branch and it is extracted from the MSc thesis of Fatemeh Omidi.
Ethical statement
This study was performed under the Declaration of Helsinki for medical research involving human subjects and received approval from the Ethics Committee of Islamic Azad University, Chalus Branch, Iran (Ethical approval code: 1401.018).
Conflicts of interest
The authors declare no conflict of interest.
Author contributions
LF contributed to study concept and edited the final manuscript. FO performed laboratory examinations and interpreted the data. All authors read and approved the final manuscript.
Type of Article: Original article |
Subject:
Health
Received: 2024/04/13 | Accepted: 2024/06/26 | Published: 2024/12/29
Received: 2024/04/13 | Accepted: 2024/06/26 | Published: 2024/12/29
References
1. Walas N, Slown S, Amato HK, Lloyd T, Bender M, Varghese V, et al. The role of plasmids in carbapenem resistant E. coli in Alameda County, California. BMC Microbiol. 2023;23(1):147. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Hosseinpour I, Fozouni L, Khademi M, Movaghari M, Akhoondi MM. The Impact of Gold Nanoparticle Susceptibility on Drug Resistance Phenotypes in Uropathogenic Escherichia coli. JoMMID. 2023;11(3):155-61. [View at Publisher] [DOI] [Google Scholar]
3. Mardani S, Fozouni L , Najafpour Gh . Zinc Oxide Nanoparticles: A Promising Solution for Controlling the Growth of Gentamicin-Resistant Uropathogenic Escherichia coli. IEM. 2022;8(2):99-106. [View at Publisher] [DOI] [Google Scholar]
4. Shahandeh Z, Sadighian F, Kalantrai N. Prevalence Escherichia coli, Klebsiella and Enterobacter Species and AmpC-producing Enterobacteriaceae in Clinical Specimens of Hospitals Affiliated to Babol University of Medical Sciences, Iran using Phenotypic and Molecular Methods. Iran J Med Microbiol. 2022;16(3):212-20. [View at Publisher] [DOI] [Google Scholar]
5. Huang E, yang xu, Leighton E, Li X. Carbapenem resistance in the food supply chain. J Food Prot. 2023;86(7):100108. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Sawa T, Kooguch K, Moriyama K. Molecular diversity of extended-spectrum β-lactamases and carbapenemases, and antimicrobial resistance. J Intensive Care. 2020;8:13. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Hsueh SC, Chao CM, Wang CY, Lai CC, Chen CH. Clinical efficacy and safety of cefiderocol in the treatment of acute bacterial infections: A systematic review and meta-analysis of randomised controlled trials. J Glob Antimicrob Resist. 2021;24:376-82. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Lee YR, Yeo S. Cefiderocol, a New Siderophore Cephalosporin for the Treatment of Complicated Urinary Tract Infections Caused by Multidrug-Resistant Pathogens: Preclinical and Clinical Pharmacokinetics, Pharmacodynamics, Efficacy and Safety. Clin Drug Investig. 2020;40(10):901-13. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Sato T, Yamawaki K. Cefiderocol: Discovery, Chemistry, and In Vivo Profiles of a Novel Siderophore Cephalosporin. Clin Infect Dis. 2019;69(Suppl 7):S538-43. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Wu JY, Srinivas P, Pogue JM. Cefiderocol: A Novel Agent for the Management of Multidrug-Resistant Gram-Negative Organisms. Infect Dis Ther. 2020;9(1):17-40. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Ghotaslou R, Sadeghi MR, Akhi MT, Hasani A, Asgharzadeh M. Prevalence and Antimicrobial Susceptibility Patterns of ESBL, AmpC and Carbapenemase-producing Enterobactericeae Isolated from Hospitalized Patients in Azerbaijan, Iran. Iran J Pharm Res. 2018;17(Suppl):79-88. [View at Publisher] [PMID] [Google Scholar]
12. CLSI Publishes M100-Performance standards for antimicrobial susceptibility testing: 31st ed. USA:Clinical and Laboratory Standards Institute;2021. [View at Publisher]
13. Fazeli H, Norouzi-Barough M, Ahadi AM, Shokri D, Solgi H. Detection of New Delhi Metallo-Beta-Lactamase-1 (NDM-1) in carbapenem- resistant Klebsiella pneumoniae isolated from a university hospital in Iran. Hippokratia. 2015;19(3):205-09. [View at Publisher] [PMID] [Google Scholar]
14. Zhang LP, Xue WC, Meng DY. First report of New Delhi metallo-β-lactamase 5 (NDM-5)-producing Escherichia coli from blood cultures of three leukemia patients. Int J Infect Dis. 2016;42:45-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Ripabelli G, Sammarco ML, Scutellà M, Felice V, Tamburro M. Carbapenem-Resistant KPC- and TEM-Producing Escherichia coli ST131 Isolated from a Hospitalized Patient with Urinary Tract Infection: First Isolation in Molise Region, Central Italy, July 2018. Microb Drug Resist . 2020;26(1):38-45. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Murugan MS, Sinha DK, Vinodh Kumar OR, Yadav AK, Pruthvishree BS, Vadhana P, et al. Epidemiology of carbapenem-resistant Escherichia coli and first report of blaVIM carbapenemases gene in calves from India. Epidemiol Infect. 2019;147:e159. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Gurung S, Kafle S, Dhungel B, Adhikari N, Shrestha UT, Adhikari B, et al. Detection of OXA-48 Gene in Carbapenem-Resistant Escherichia coli and Klebsiella pneumoniae from Urine Samples. Infect Drug Resist. 2020;13:2311-21. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Moemen D, Masallat DT. Prevalence and characterization of carbapenem-resistant Klebsiella pneumoniae isolated from intensive care units of Mansoura University hospitals. Egypt J Basic Appl Sci .2017;4(1):37-41. [View at Publisher] [DOI] [Google Scholar]
19. Padovani M, Bertelli A, Corbellini S, Piccinelli G, Gurrieri F, De Francesco MA. In Vitro Activity of Cefiderocol on Multiresistant Bacterial Strains and Genomic Analysis of Two Cefiderocol Resistant Strains. Antibiotics (Basel). 2023;12(4):785. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Falagas M, Skalidis T, Vardakas K, Legakis N, Tsiplakou S, Papaioannou V, et al. Activity of cefiderocol (S-649266) against carbapenem-resistant Gram-negative bacteria collected from inpatients in Greek hospitals. J Antimicrob Chemother. 2017;72(6):1704-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Alzayer M, Alghoribi MF, Alalwan B, Alreheli A, Aljohani S, Bosaeed M, et al. In vitro activity of cefiderocol against clinically important carbapenem non-susceptible Gram-negative bacteria from Saudi Arabia. J Glob Antimicrob Resist. 2023:32:176-80. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Wang Y, Li Y, Zhao J, Guan J, Ni W, Gao Z. Susceptibility of cefiderocol and other antibiotics against carbapenem-resistant, Gram-negative bacteria. Ann Transl Med. 2022;10(5):261. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |