
Thu, Oct 2, 2025
Volume 18, Issue 1 (Jan-Feb 2024)
mljgoums 2024, 18(1): 23-26 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shirdel Abdolmaleki A, Rafati Zomorodi A, Motamedifar M, Malekzadegan Y. Antimicrobial susceptibility patterns in Escherichia coli isolates from Hospital-acquired urinary tract infections. mljgoums 2024; 18 (1) :23-26
URL: http://mlj.goums.ac.ir/article-1-1521-en.html
URL: http://mlj.goums.ac.ir/article-1-1521-en.html
Abolfazl Shirdel Abdolmaleki1 

 , Abolfazl Rafati Zomorodi1 , Mohammad Motamedifar2 , Yalda Malekzadegan3
, Abolfazl Rafati Zomorodi1 , Mohammad Motamedifar2 , Yalda Malekzadegan3
, Abolfazl Rafati Zomorodi1 , Mohammad Motamedifar2 , Yalda Malekzadegan3
1- Department of Bacteriology and Virology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
2- Department of Bacteriology and Virology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran ,motamedm@sums.ac.ir
3- Department of Microbiology, Saveh University of Medical Sciences, Saveh, Iran
2- Department of Bacteriology and Virology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; HIV/AIDS Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran ,
3- Department of Microbiology, Saveh University of Medical Sciences, Saveh, Iran
Full-Text [PDF 556 kb]
(1006 Downloads)
| Abstract (HTML) (3800 Views)
Full-Text: (957 Views)
Introduction
In developing countries (such as Iran), hospital-acquired infections (HAIs) are a major cause of adverse events and mortality for hospitalized patients, as well as reduced quality of life for hospitalized individuals (1). They result in longer hospital stays, higher medical costs, improper broad-spectrum antibiotic use, and multiple antibiotic resistance. Previous studies have shown that the HAI prevalence differs in Iranian hospitals based on the prevalence and antimicrobial resistance. Urinary tract infections (UTIs) caused by Escherichia coli are reported chiefly as predominant HAIs (2). Urinary tract infections affect from 5% to 15% of hospitalized patients in regular wards and more than half of intensive care unit (ICU) patients. Earlier investigations in Iran suggested the high frequency of HA-UTIs, especially among ICU-admitted patients, which is twice as common as in other countries (3). Previous studies have also reported that HA-UTIs are the most common HAI in Shiraz (4, 5).
While antimicrobial resistance has increased significantly worldwide, UTI treatment leads to abundant antibiotic application in hospitals and communities, continuously developing multidrug resistance (MDR). Multidrug resistance is defined as acquired non-susceptibility to at least 1 drug in 3 or more classes of antimicrobials, based on the European Centre for Disease Prevention and Control (ECDC) (6). However, uncomplicated UTIs can cause dangerous complications (such as sepsis, pneumonia, bacteremia, and surgical site infections) due to the deficiency of proper diagnosis and treatment guidelines (7).
According to international guidelines, empiric treatment accrues for UTI patients with first-line antibiotics (nitrofurantoin, trimethoprim-sulfamethoxazole, fosfomycin, or pivmecillinam), but there is a lack of consensus among guidelines about the consumption of fluoroquinolones (FQs) (8). Although FQs are prescribed as first-line treatment options in Asia, the US and European guidelines emphasize using FQs only when there are no other options (9, 10). Therefore, the prevalence of FQ-resistant E. coli is variable in different parts of the world, ranging from 50% to 98% of strains causing catheter related UTIs (CR-UTIs) and 20% of all HA-UTIs (11). On the other hand, a decrease in susceptibility to the β-lactam family among E. coli isolates from UTIs becomes a concern (12).
The rate of susceptibility of E. coli isolates from UTIs to antibiotics has varied over time, across geographical locations, or even from 1 institute or hospital to another in the same city. Hence, it seems essential for all institutes or hospitals to maintain continuous antimicrobial stewardship by assessing antimicrobial susceptibility patterns (ASP) among E. coli isolates from HA-UTIs.
The present investigation aimed to demonstrate a comprehensive investigation of ASP among E. coli isolates from HA-UTIs in Nemazee Hospital, the biggest hospital in southwest Iran.
Methods
The current cross-sectional study was conducted from 2018 to 2019 at Nemazee Hospital, affiliated with Shiraz University of Medical Sciences, Shiraz, southwest Iran. Escherichia coli isolates were collected from hospitalized patients with symptoms of UTIs. The isolates were collected from patients who acquired UTI within 48-72 h after admission to the hospital.
The isolates were identified by standard biochemical tests, as earlier described by Aflakian, Rad (13), including Triple Sugar Iron agar (TSI), Simmons' citrate agar, Christensen's urea agar, Indole test, Methyl red, and Voges-Proskauer tests. The E. coli strains were stored in Trypticase Soy Broth (TSB) with 15% glycerol at -70 ℃ for prolonged preservation.
The evaluation of antimicrobial susceptibility was conducted with the Kirby-Bauer disk diffusion method as recommended by the Clinical and Laboratory Standard Institute (CLSI) 2020 (14) for 12 antibiotic disks as follows: cefixime (5 µg), ceftriaxone (30 µg), cephalexin (30 µg), cefotaxime (30 µg), ciprofloxacin (5 µg), norfloxacin (10 µg), nalidixic acid (30 µg), amikacin (30 µg), gentamicin (10 µg), tetracycline (30 µg), nitrofurantoin (300 µg), trimethoprim-sulfamethoxazole (1.25/23.75 µg).
Analyses were performed using SPSS version 22.0 (IBM Corp, USA). The results are presented as descriptive statistics in terms of relative frequency. Values were expressed as mean ± SD (continuous variables) or group percentages (categorical variables). A chi-square statistical test was performed to analyze the data, and P ≤ 0.05 was considered statistically significant.
Results
A total of 1910 out of 44 657 urine cultures for 2 years (2018 and 2019) were reported positive for E. coli. The mean age of participants was 52.78 years (SD = 29.00), and 1215 (63.6%) of those were women, with a mean age of 50.65 years (SD = 28.62).
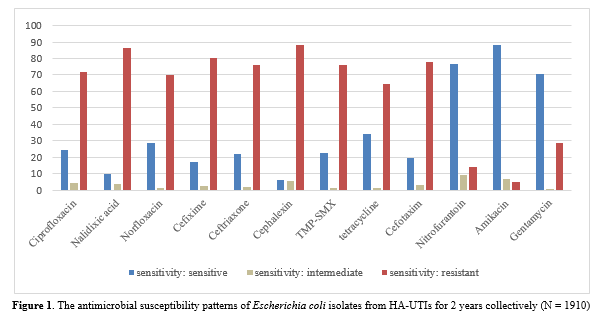
The results showed the highest resistance against cephalexin (87.9%) and nalidixic acid (86.1%), followed by cefixime (80.1%), cefotaxime (78%), trimethoprim-sulfamethoxazole (75.8%), and ciprofloxacin (71.5%). On the other hand, the lowest resistance was recorded for amikacin (88.3%), nitrofurantoin (76.8%), and gentamycin (70.6%). Figure 1 shows the frequency of antimicrobial resistance. In addition, 1624 out of 1910 isolates were MDR.
Based on the chi-square test, the rate of resistance to ciprofloxacin (P = 0.004), norfloxacin (P = 0.008), tetracycline (P = 0.038), cefotaxime (P = 0.015), and nitrofurantoin (P < 0.001) has significantly increased during these 2 years. The results of assessing antimicrobial resistance are shown in Table 1 for different years.
The highest resistance rate was observed for nalidixic acid in surgical wards (95.3%) and cephalexin in adults’ ICU (90.8%). Also, amikacin had the lowest resistance among the isolates obtained from all wards. Table 2 shows the distribution of antimicrobial resistance according to hospitalized wards.
Discussion
It is estimated that UTIs represent about 10-20% of infections in primary care units and 30-40% in hospitals; on the whole, over 150 million cases of UTI diseases have been reported per year worldwide, resulting in 6 billion US dollars in treatment costs. The increasing number of MDR E. coli isolates causing UTI is of global significance because they lead to clinical and economic burdens (15).
In the current study, as expected, the UTI prevalence was observed more among women (64%); this finding was consistent with previous reports (16). This phenomenon might be explained by the discrepancy in perineal anatomy in men and women, including shortness of the urethra and closeness of the urethral meatus to the anus, spermicide-based contraception, and a history of UTI in their mothers (17).
The results revealed a significantly increased resistant rate of isolates against β-lactam family antibiotics, including cephalexin (87.9%) and cefixime (80.1%). This is consistent with previous surveys by Neupane, Pant (18) in Nepal and Hossain, Ahmad (19) in Bangladesh; they reported a high frequency of cephalexin resistance phenotype (84.1%). In comparison, the rate of resistant isolates against cefixime was 75.5% and 57.7%, respectively, which is not consistent with our findings. Remarkably, cefotaxime resistance increased statistically during these 2 years; the frequency of resistance against cefotaxime was 69.2% and 77.8% in 2018 and 2019, respectively. A comprehensive assessment in Korea revealed a rising trend in cefotaxime resistance from 2008 to 2017, from 4.5% to 32% (20). Yet, our finding was higher than that for this study and another in Nepal, with a 44.38% resistance frequency (21). Nonetheless, the current observation was in line with previous results by Pouladfar and Basiratnia (22), reporting 63.4% resistance to cefotaxime among UTI patients hospitalized at Nemazee Hospital in Shiraz. Although these results differ from some published studies (23, 24), which reported a lower frequency of resistance, this controversy could be attributed to the lack of effective antimicrobial stewardship in Iran. Generally, increasing resistance against β-lactam antibiotics, especially third-generation cephalosporins, is related to widespread extended-spectrum beta-lactamase (ESBL) producing E. coli; subsequently, carbapenems are prescribed with high efficacy for UTIs (25). However, the widespread dissemination of carbapenemase-producing E. coli is a major concern.
Interestingly, the low frequency of nitrofurantoin resistance (13.8%) was reduced compared to an earlier survey in Shiraz (22). Several reasons could be involved in this event, such as using nitrofurantoin only in mild UTI cases or limiting nitrofurantoin through its side effects. Nevertheless, a review article by Giske (26) revealed lower nitrofurantoin resistance in Europe (1%). Quinolone resistance was significantly increased for nalidixic acid (86.1%), ciprofloxacin (71.5%), and norfloxacin (70.2%) among isolates. Based on comparisons of the distribution of quinolone-resistant E. coli in India, the USA, and Egypt, differences have been determined region by region in this case (27-29). A prior study by Mirzaii and Jamshidi (30) reported an 87% resistance rate to nalidixic acid in Shahroud, Iran. These values did not correlate with another survey by Norouzian and Shahrokhi (31) in Tehran, reporting a resistance prevalence for nalidixic acid, ciprofloxacin, and norfloxacin at 67.8%, 48.7%, and 44.1%, respectively. The controversy surrounding the use of quinolone antibiotics might lead to differences in quinolone resistance prevalence between countries or even different geographical areas in the same country. Several investigations have indicated AMR development caused by mobile-genetic elements, such as plasmids, transposons, and gene cassette-integrons, transferred among the Enterobacteriaceae family, especially E. coli strains. Therefore, increasing resistance frequency against β-lactams, nitrofurantoin, and quinolone antibiotics during these 2 years might be the result of spreading the plasmid-mediated resistance among E. coli strains.
In total, 1624 (85%) of isolates (714 and 910 in 2018 and 2019, respectively) were identified as MDR, indicating resistance to at least 1 antimicrobial agent in 3 different antibiotic families. Compared with earlier studies in other Iranian cities (Hamedan, Kashan, and Yasuj), it was 64%, 74%, and 79% in 2015 and 2016, respectively. Thus, an increasing trend in MDR among E. coli isolates from UTI patients was reported (32-34). Also, Naziri et al. reported 93.6% MDR isolates in Shiraz in 2020 (35). However, the frequency of MDR isolates in other countries (in Mexico, 63%; in India and Nepal, 65%; in Egypt, 73%) was lower than the findings in the current study (36-39). On the other hand, the observation of 90% MDR by Chowdhury et al. in Bangladesh was consistent with our results (40). Unfortunately, it was impossible to analyze more data from other Shiraz hospitals; thus, further studies are essential to determine ASP for E. coli isolates from UTI patients admitted to different hospitals.
Conclusion
The current study provides further evidence for an increase in AMR and MDR isolates among E. coli isolates from HA-UTIs due to excessive and improper antibiotic consumption. In addition, these measures emphasize the proper use of antibiotics and infection-control measures to prevent resistant strains. The administration of appropriate antibiotic therapy and the implementation of techniques for identifying resistant organisms as early as possible need to be simplified.
Acknowledgement
The authors thank all hospital staff who collaborated on this study.
Funding sources
This article was extracted from Dr Abolfazl Shirdel Abdolmaleki's MD thesis and was financially supported by Shiraz University of Medical Sciences (Grant number 21469).
Ethical statement
The current study was approved by the Research Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1399.163). Also, all patients’ information remains confidential. All patients have signed an informed consent form.
Conflicts of interest
The authors declare that there is no conflict of interest.
Author contributions
A.S. and A.R.Z. collected and curated the data and contributed to the guide and concept of the study and statistical analysis; Y.M. contributed to writing the manuscript; M.M. administrated the project, led the group, and edited the draft of the manuscript. All authors read and approved the final manuscript.
In developing countries (such as Iran), hospital-acquired infections (HAIs) are a major cause of adverse events and mortality for hospitalized patients, as well as reduced quality of life for hospitalized individuals (1). They result in longer hospital stays, higher medical costs, improper broad-spectrum antibiotic use, and multiple antibiotic resistance. Previous studies have shown that the HAI prevalence differs in Iranian hospitals based on the prevalence and antimicrobial resistance. Urinary tract infections (UTIs) caused by Escherichia coli are reported chiefly as predominant HAIs (2). Urinary tract infections affect from 5% to 15% of hospitalized patients in regular wards and more than half of intensive care unit (ICU) patients. Earlier investigations in Iran suggested the high frequency of HA-UTIs, especially among ICU-admitted patients, which is twice as common as in other countries (3). Previous studies have also reported that HA-UTIs are the most common HAI in Shiraz (4, 5).
While antimicrobial resistance has increased significantly worldwide, UTI treatment leads to abundant antibiotic application in hospitals and communities, continuously developing multidrug resistance (MDR). Multidrug resistance is defined as acquired non-susceptibility to at least 1 drug in 3 or more classes of antimicrobials, based on the European Centre for Disease Prevention and Control (ECDC) (6). However, uncomplicated UTIs can cause dangerous complications (such as sepsis, pneumonia, bacteremia, and surgical site infections) due to the deficiency of proper diagnosis and treatment guidelines (7).
According to international guidelines, empiric treatment accrues for UTI patients with first-line antibiotics (nitrofurantoin, trimethoprim-sulfamethoxazole, fosfomycin, or pivmecillinam), but there is a lack of consensus among guidelines about the consumption of fluoroquinolones (FQs) (8). Although FQs are prescribed as first-line treatment options in Asia, the US and European guidelines emphasize using FQs only when there are no other options (9, 10). Therefore, the prevalence of FQ-resistant E. coli is variable in different parts of the world, ranging from 50% to 98% of strains causing catheter related UTIs (CR-UTIs) and 20% of all HA-UTIs (11). On the other hand, a decrease in susceptibility to the β-lactam family among E. coli isolates from UTIs becomes a concern (12).
The rate of susceptibility of E. coli isolates from UTIs to antibiotics has varied over time, across geographical locations, or even from 1 institute or hospital to another in the same city. Hence, it seems essential for all institutes or hospitals to maintain continuous antimicrobial stewardship by assessing antimicrobial susceptibility patterns (ASP) among E. coli isolates from HA-UTIs.
The present investigation aimed to demonstrate a comprehensive investigation of ASP among E. coli isolates from HA-UTIs in Nemazee Hospital, the biggest hospital in southwest Iran.
Methods
The current cross-sectional study was conducted from 2018 to 2019 at Nemazee Hospital, affiliated with Shiraz University of Medical Sciences, Shiraz, southwest Iran. Escherichia coli isolates were collected from hospitalized patients with symptoms of UTIs. The isolates were collected from patients who acquired UTI within 48-72 h after admission to the hospital.
The isolates were identified by standard biochemical tests, as earlier described by Aflakian, Rad (13), including Triple Sugar Iron agar (TSI), Simmons' citrate agar, Christensen's urea agar, Indole test, Methyl red, and Voges-Proskauer tests. The E. coli strains were stored in Trypticase Soy Broth (TSB) with 15% glycerol at -70 ℃ for prolonged preservation.
The evaluation of antimicrobial susceptibility was conducted with the Kirby-Bauer disk diffusion method as recommended by the Clinical and Laboratory Standard Institute (CLSI) 2020 (14) for 12 antibiotic disks as follows: cefixime (5 µg), ceftriaxone (30 µg), cephalexin (30 µg), cefotaxime (30 µg), ciprofloxacin (5 µg), norfloxacin (10 µg), nalidixic acid (30 µg), amikacin (30 µg), gentamicin (10 µg), tetracycline (30 µg), nitrofurantoin (300 µg), trimethoprim-sulfamethoxazole (1.25/23.75 µg).
Analyses were performed using SPSS version 22.0 (IBM Corp, USA). The results are presented as descriptive statistics in terms of relative frequency. Values were expressed as mean ± SD (continuous variables) or group percentages (categorical variables). A chi-square statistical test was performed to analyze the data, and P ≤ 0.05 was considered statistically significant.
Results
A total of 1910 out of 44 657 urine cultures for 2 years (2018 and 2019) were reported positive for E. coli. The mean age of participants was 52.78 years (SD = 29.00), and 1215 (63.6%) of those were women, with a mean age of 50.65 years (SD = 28.62).
The results showed the highest resistance against cephalexin (87.9%) and nalidixic acid (86.1%), followed by cefixime (80.1%), cefotaxime (78%), trimethoprim-sulfamethoxazole (75.8%), and ciprofloxacin (71.5%). On the other hand, the lowest resistance was recorded for amikacin (88.3%), nitrofurantoin (76.8%), and gentamycin (70.6%). Figure 1 shows the frequency of antimicrobial resistance. In addition, 1624 out of 1910 isolates were MDR.
Based on the chi-square test, the rate of resistance to ciprofloxacin (P = 0.004), norfloxacin (P = 0.008), tetracycline (P = 0.038), cefotaxime (P = 0.015), and nitrofurantoin (P < 0.001) has significantly increased during these 2 years. The results of assessing antimicrobial resistance are shown in Table 1 for different years.
Table 1. The prevalence of antimicrobial resistance of Escherichia coli isolates from HA-UTIs Table 2. Distribution of antimicrobial susceptibility patterns of Escherichia coli isolates from HA-UTIs according to Hospitals’ ward over 2 years 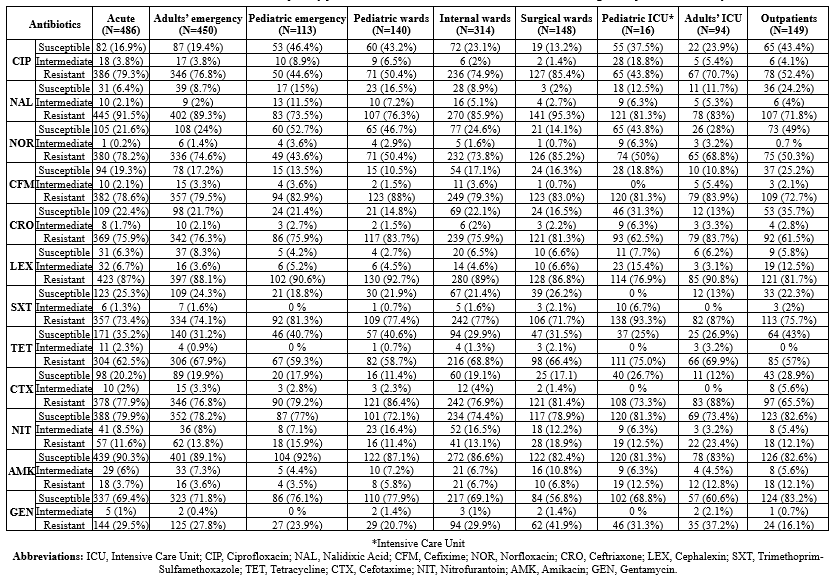 |
Discussion
It is estimated that UTIs represent about 10-20% of infections in primary care units and 30-40% in hospitals; on the whole, over 150 million cases of UTI diseases have been reported per year worldwide, resulting in 6 billion US dollars in treatment costs. The increasing number of MDR E. coli isolates causing UTI is of global significance because they lead to clinical and economic burdens (15).
In the current study, as expected, the UTI prevalence was observed more among women (64%); this finding was consistent with previous reports (16). This phenomenon might be explained by the discrepancy in perineal anatomy in men and women, including shortness of the urethra and closeness of the urethral meatus to the anus, spermicide-based contraception, and a history of UTI in their mothers (17).
The results revealed a significantly increased resistant rate of isolates against β-lactam family antibiotics, including cephalexin (87.9%) and cefixime (80.1%). This is consistent with previous surveys by Neupane, Pant (18) in Nepal and Hossain, Ahmad (19) in Bangladesh; they reported a high frequency of cephalexin resistance phenotype (84.1%). In comparison, the rate of resistant isolates against cefixime was 75.5% and 57.7%, respectively, which is not consistent with our findings. Remarkably, cefotaxime resistance increased statistically during these 2 years; the frequency of resistance against cefotaxime was 69.2% and 77.8% in 2018 and 2019, respectively. A comprehensive assessment in Korea revealed a rising trend in cefotaxime resistance from 2008 to 2017, from 4.5% to 32% (20). Yet, our finding was higher than that for this study and another in Nepal, with a 44.38% resistance frequency (21). Nonetheless, the current observation was in line with previous results by Pouladfar and Basiratnia (22), reporting 63.4% resistance to cefotaxime among UTI patients hospitalized at Nemazee Hospital in Shiraz. Although these results differ from some published studies (23, 24), which reported a lower frequency of resistance, this controversy could be attributed to the lack of effective antimicrobial stewardship in Iran. Generally, increasing resistance against β-lactam antibiotics, especially third-generation cephalosporins, is related to widespread extended-spectrum beta-lactamase (ESBL) producing E. coli; subsequently, carbapenems are prescribed with high efficacy for UTIs (25). However, the widespread dissemination of carbapenemase-producing E. coli is a major concern.
Interestingly, the low frequency of nitrofurantoin resistance (13.8%) was reduced compared to an earlier survey in Shiraz (22). Several reasons could be involved in this event, such as using nitrofurantoin only in mild UTI cases or limiting nitrofurantoin through its side effects. Nevertheless, a review article by Giske (26) revealed lower nitrofurantoin resistance in Europe (1%). Quinolone resistance was significantly increased for nalidixic acid (86.1%), ciprofloxacin (71.5%), and norfloxacin (70.2%) among isolates. Based on comparisons of the distribution of quinolone-resistant E. coli in India, the USA, and Egypt, differences have been determined region by region in this case (27-29). A prior study by Mirzaii and Jamshidi (30) reported an 87% resistance rate to nalidixic acid in Shahroud, Iran. These values did not correlate with another survey by Norouzian and Shahrokhi (31) in Tehran, reporting a resistance prevalence for nalidixic acid, ciprofloxacin, and norfloxacin at 67.8%, 48.7%, and 44.1%, respectively. The controversy surrounding the use of quinolone antibiotics might lead to differences in quinolone resistance prevalence between countries or even different geographical areas in the same country. Several investigations have indicated AMR development caused by mobile-genetic elements, such as plasmids, transposons, and gene cassette-integrons, transferred among the Enterobacteriaceae family, especially E. coli strains. Therefore, increasing resistance frequency against β-lactams, nitrofurantoin, and quinolone antibiotics during these 2 years might be the result of spreading the plasmid-mediated resistance among E. coli strains.
In total, 1624 (85%) of isolates (714 and 910 in 2018 and 2019, respectively) were identified as MDR, indicating resistance to at least 1 antimicrobial agent in 3 different antibiotic families. Compared with earlier studies in other Iranian cities (Hamedan, Kashan, and Yasuj), it was 64%, 74%, and 79% in 2015 and 2016, respectively. Thus, an increasing trend in MDR among E. coli isolates from UTI patients was reported (32-34). Also, Naziri et al. reported 93.6% MDR isolates in Shiraz in 2020 (35). However, the frequency of MDR isolates in other countries (in Mexico, 63%; in India and Nepal, 65%; in Egypt, 73%) was lower than the findings in the current study (36-39). On the other hand, the observation of 90% MDR by Chowdhury et al. in Bangladesh was consistent with our results (40). Unfortunately, it was impossible to analyze more data from other Shiraz hospitals; thus, further studies are essential to determine ASP for E. coli isolates from UTI patients admitted to different hospitals.
Conclusion
The current study provides further evidence for an increase in AMR and MDR isolates among E. coli isolates from HA-UTIs due to excessive and improper antibiotic consumption. In addition, these measures emphasize the proper use of antibiotics and infection-control measures to prevent resistant strains. The administration of appropriate antibiotic therapy and the implementation of techniques for identifying resistant organisms as early as possible need to be simplified.
Acknowledgement
The authors thank all hospital staff who collaborated on this study.
Funding sources
This article was extracted from Dr Abolfazl Shirdel Abdolmaleki's MD thesis and was financially supported by Shiraz University of Medical Sciences (Grant number 21469).
Ethical statement
The current study was approved by the Research Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1399.163). Also, all patients’ information remains confidential. All patients have signed an informed consent form.
Conflicts of interest
The authors declare that there is no conflict of interest.
Author contributions
A.S. and A.R.Z. collected and curated the data and contributed to the guide and concept of the study and statistical analysis; Y.M. contributed to writing the manuscript; M.M. administrated the project, led the group, and edited the draft of the manuscript. All authors read and approved the final manuscript.
Research Article: Research Article |
Subject:
bacteriology
Received: 2022/05/22 | Accepted: 2023/12/5 | Published: 2024/01/21 | ePublished: 2024/01/21
Received: 2022/05/22 | Accepted: 2023/12/5 | Published: 2024/01/21 | ePublished: 2024/01/21
References
1. Izadi N, Eshrati B, Etemad K, Mehrabi Y, Hashemi-Nazari S-S. Rate of the incidence of hospital-acquired infections in Iran based on the data of the national nosocomial infections surveillance. New Microbes New Infect. 2020;38:100768. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Nouri F, Karami P, Zarei O, Kosari F, Alikhani MY, Zandkarimi E, et al. Prevalence of common nosocomial infections and evaluation of antibiotic resistance patterns in patients with secondary infections in Hamadan, Iran. Infect Drug Resist. 2020;13:2365-74. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Faezi Ghasemi M, Dibadji SN. Prevalence of blaoxa-1 and blashv Genes in E. coli Isolates from Hospitalized Patients in Rasht. Med Laborator J. 2016;10(5):65-70. [View at Publisher] [DOI] [Google Scholar]
4. Dashti AS, Kadivar MR, Tabatabai A, Zand F, Salami S, Ezadpanah S, et al. Prevalence of Healthcare-Associated Infections in Pediatric Wards of Nemazee Teaching Hospital in Shiraz: A Comparison with the Whole Hospital. Arch Pediatr Infect Dis. 2019;7(1). [View at Publisher] [DOI] [Google scholar]
5. Hassanzadeh P, Motamedifar M, Hadi N. Prevalent bacterial infections in intensive care units of Shiraz University of medical sciences teaching hospitals, Shiraz, Iran. Jpn J Infect Dis. 2009;62(4):249-53. [View at Publisher] [DOI] [PMID] [Google scholar]
6. Wolfensberger A, Kuster SP, Marchesi M, Zbinden R, Hombach M. The effect of varying multidrug-resistence (MDR) definitions on rates of MDR gram-negative rods. Antimicrob Resist Infect Control. 2019;8(1):1-9. [View at Publisher] [DOI] [PMID] [Google scholar]
7. Gonzalez M, Razzano D, Ebid A, Schubert FD. Clinical and Antibiotic Management of Urinary Tract Infections Pre-and Postimplementation of the CLINITEK AUWi System From Siemens to Screen Out Negative Urine Samples Submitted for Culture: A Retrospective Cohort Study. Lab Med. 2018;49(1):18-24. [View at Publisher] [DOI] [PMID] [Google scholar]
8. Lopez AMCO, Tan CJL, Yabon AS, Masbang AN. Symptomatic treatment (using NSAIDS) versus antibiotics in uncomplicated lower urinary tract infection: a meta-analysis and systematic review of randomized controlled trials. BMC Infecti Dis. 2021;21(1):619. [View at Publisher] [DOI] [PMID] [Google scholar]
9. Stapleton AE, Wagenlehner FM, Mulgirigama A, Twynholm M. E coli Resistance to Fluoroquinolones in Community-Acquired Uncomplicated Urinary Tract Infection In Women: A Systematic Review. Antimicrob Agents Chemother. 2020;64(10):e00862-20. [View at Publisher] [DOI] [PMID] [Google scholar]
10. Rastogi R, Martinez KA, Gupta N, Rood M, Rothberg MB. Management of urinary tract infections in direct to consumer telemedicine. J Gen Intern Med. 2020;35(3):643-8. [View at Publisher] [DOI] [PMID] [Google scholar]
11. Vieira DC, Lima WG, de Paiva MC. Plasmid-mediated quinolone resistance (PMQR) among Enterobacteriales in Latin America: a systematic review. Mol Biol Rep. 2020;47(2):1471-83. [View at Publisher] [DOI] [PMID] [Google scholar]
12. Taha SA, Omar HH. Characterization of plasmid-mediated qnrA and qnrB genes among Enterobacteriaceae strains: quinolone resistance and ESBL production in Ismailia, Egypt. Egypt J Med Hum Genet. 2019;20(1):1-7. [View at Publisher] [DOI] [Google scholar]
13. Aflakian F, Rad M, Salimizand H, Nemati A, Zomorodi AR. Detection of virulence genes and determination of the antimicrobial susceptibility of Escherichia coli isolates with mastitis in Mashhad, Iran-a short communication. Veterinarski arhiv. 2022;92(4):525-30. [View at Publisher] [DOI] [Google scholar]
14. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2020. [View at Publisher] [Google scholar]
15. Lee DS, Lee S-J, Choe HS. Community-acquired urinary tract infection by Escherichia coli in the era of antibiotic resistance. BioMed Res Int. 2018;2018:7656752. [View at Publisher] [DOI] [PMID] [Google scholar]
16. Sako A, Yasunaga H, Matsui H, Fushimi K, Yanai H, Gu Y, et al. Hospitalization for urinary tract infections in Japan, 2010-2015: a retrospective study using a national inpatient database. BMC Infect Dis. 2021;21(1):1048. [View at Publisher] [DOI] [PMID] [Google scholar]
17. Asma B, Vicky L, Stephanie D, Yves D, Amy H, Sylvie D. Standardised high dose versus low dose cranberry Proanthocyanidin extracts for the prevention of recurrent urinary tract infection in healthy women [PACCANN]: a double blind randomised controlled trial protocol. BMC Urol. 2018;18(1):29. [View at Publisher] [DOI] [PMID] [Google scholar]
18. Neupane S, Pant ND, Khatiwada S, Chaudhary R, Banjara MR. Correlation between biofilm formation and resistance toward different commonly used antibiotics along with extended spectrum beta lactamase production in uropathogenic Escherichia coli isolated from the patients suspected of urinary tract infections visiting Shree Birendra Hospital, Chhauni, Kathmandu, Nepal. Antimicrob Resist Infect Control. 2016;5(1):5. [View at Publisher] [DOI] [PMID] [Google scholar]
19. Hossain A, Hossain SA, Fatema AN, Wahab A, Alam MM, Islam MN, et al. Age and gender-specific antibiotic resistance patterns among Bangladeshi patients with urinary tract infection caused by Escherichia coli. Heliyon. 2020;6(6):e04161. [View at Publisher] [DOI] [PMID] [Google scholar]
20. Kim YJ, Lee J-M, Cho J, Lee J. Change in the annual antibiotic susceptibility of Escherichia coli in community-onset urinary tract infection between 2008 and 2017 in a tertiary care hospital in Korea. J Korean Med Sci. 2019;34(34):e228. [View at Publisher] [DOI] [PMID] [Google scholar]
21. Shakya P, Shrestha D, Maharjan E, Sharma VK, Paudyal R. ESBL production among E. coli and Klebsiella spp. causing urinary tract infection: a hospital based study. Open Microbiol J. 2017;11:23-30. [View at Publisher] [DOI] [PMID] [Google scholar]
22. Pouladfar G, Basiratnia M, Anvarinejad M, Abbasi P, Amirmoezi F, Zare S. The antibiotic susceptibility patterns of uropathogens among children with urinary tract infection in Shiraz. Medicine (Baltimore). 2017;96(37):e7834. [View at Publisher] [DOI] [PMID] [Google scholar]
23. Park K-H, Oh WS, Kim ES, Park SW, Hur J-A, Kim YK, et al. Factors associated with ciprofloxacin-and cefotaxime-resistant Escherichia coli in women with acute pyelonephritis in the emergency department. Int J Infect Dis. 2014;23:8-13. [View at Publisher] [DOI] [PMID] [Google Scholar]
24. Rossignol L, Vaux S, Maugat S, Blake A, Barlier R, Heym B, et al. Incidence of urinary tract infections and antibiotic resistance in the outpatient setting: a cross-sectional study. Infection. 2017;45(1):33-40. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Komijani M, Bouzari M, Rahimi F. Detection of TEM, SHV and CTX-M antibiotic resistance genes in Escherichia coli isolates from infected wounds. Medical Laboratory Journal. 2017;11(2):30-5. [View at Publisher] [DOI] [Google Scholar]
26. Giske C. Contemporary resistance trends and mechanisms for the old antibiotics colistin, temocillin, fosfomycin, mecillinam and nitrofurantoin. Clin Microbiol Infect. 2015;21(10):899-905. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Critchley IA, Cotroneo N, Pucci MJ, Mendes R. The burden of antimicrobial resistance among urinary tract isolates of Escherichia coli in the United States in 2017. PLoS One. 2019;14(12):e0220265. [View at Publisher] [DOI] [PMID] [Google scholar]
28. Basu S, Mukherjee M. Incidence and risk of co-transmission of plasmid-mediated quinolone resistance and extended-spectrum β-lactamase genes in fluoroquinolone-resistant uropathogenic Escherichia coli: a first study from Kolkata, India. J Glob Antimicrob Resist. 2018;14:217-23. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Esmaeel NE, Gerges MA, Hosny TA, Ali AR, Gebriel MG. Detection of chromosomal and plasmid-mediated quinolone resistance among Escherichia coli Isolated from urinary tract infection cases; Zagazig University Hospitals, Egypt. Infect Drug Resist. 2020;13:413-21. [View at Publisher] [DOI] [PMID] [Google scholar]
30. Mirzaii M, Jamshidi S, Zamanzadeh M, Marashifard M, Hosseini SAAM, Haeili M, et al. Determination of gyrA and parC mutations and prevalence of plasmid-mediated quinolone resistance genes in Escherichia coli and Klebsiella pneumoniae isolated from patients with urinary tract infection in Iran. J Glob Antimicrob Resist. 2018;13:197-200. [View at Publisher] [DOI] [PMID] [Google Scholar]
31. Norouzian H, Shahrokhi N, Sabeti S, Bouzari S, Pooya M. Evaluation of Quinolone Resistance in Escherichia coli Isolates Recovered from Urine and Feces of Patients with Acute or Recurrent Urinary Tract Infection. J Med Microbiol Infect Dis. 2019;7(4):120-6. [View at Publisher] [DOI] [Google Scholar]
32. Neamati F, Firoozeh F, Saffari M, Zibaei M. Virulence genes and antimicrobial resistance pattern in uropathogenic Escherichia coli isolated from hospitalized patients in Kashan, Iran. Jundishapur J Microbiol. 2015;8(2):e17514. [View at Publisher] [DOI] [PMID] [Google scholar]
33. Khoramrooz SS, Sharifi A, Yazdanpanah M, Hosseini SAAM, Emaneini M, Gharibpour F, et al. High frequency of class 1 integrons in Escherichia coli isolated from patients with urinary tract infections in Yasuj, Iran. Iran Red Crescent Med J. 2016;18(1):e26399. [View at Publisher] [DOI] [PMID] [Google scholar]
34. Mamani M, Nobari N, Alikhani MY, Poorolajal J. Antibacterial susceptibility of Escherichia coli among outpatients with community-acquired urinary tract infection in Hamadan, Iran. J Glob Antimicrob Resist. 2015;3(1):40-3. [View at Publisher] [DOI] [PMID] [Google Scholar]
35. Naziri Z, Derakhshandeh A, Borchaloee AS, Poormaleknia M, Azimzadeh N. Treatment failure in urinary tract infections: a warning witness for virulent multi-drug resistant ESBL-producing Escherichia coli. Infect Drug Resist. 2020;13:1839-50. [View at Publisher] [DOI] [PMID] [Google scholar]
36. Ramírez-Castillo FY, Moreno-Flores AC, Avelar-González FJ, Márquez-Díaz F, Harel J, Guerrero-Barrera AL. An evaluation of multidrug-resistant Escherichia coli isolates in urinary tract infections from Aguascalientes, Mexico: cross-sectional study. Ann Clin Microbiol Antimicrob. 2018;17(1):34. [View at Publisher] [DOI] [PMID] [Google scholar]
37. Sharma N, Gupta A, Walia G, Bakhshi R. Pattern of antimicrobial resistance of Escherichia coli isolates from urinary tract infection patients: A three year retrospective study. J Appl Pharm Sci. 2016;6(1):062-5. [View at Publisher] [DOI] [Google Scholar]
38. Pandit R, Awal B, Shrestha SS, Joshi G, Rijal BP, Parajuli NP. Extended-spectrum β-lactamase (ESBL) genotypes among multidrug-resistant uropathogenic Escherichia coli clinical isolates from a teaching hospital of Nepal. Interdiscip Perspect Infect Dis. 2020;2020:6525826. [View at Publisher] [DOI] [PMID] [Google scholar]
39. Masoud SM, El-Baky A, Mahmoud R, Aly SA, Ibrahem RA. Co-existence of certain ESBLs, MBLs and plasmid mediated quinolone resistance genes among MDR E. coli isolated from different clinical specimens in Egypt. Antibiotics. 2021;10(7):835. [View at Publisher] [DOI] [PMID] [Google scholar]
40. Chowdhury N, Suhani S, Purkaystha A, Begum MK, Raihan T, Alam MJ, et al. Identification of AcrAB-TolC efflux pump genes and detection of mutation in efflux repressor AcrR from omeprazole responsive multidrug-resistant Escherichia coli isolates causing urinary tract infections. Microbiol Insights. 2019;12:1178636119889629. [View at Publisher] [DOI] [PMID] [Google scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.