
Sun, Aug 3, 2025
Volume 19, Issue 2 (Mar-Apr 2025)
mljgoums 2025, 19(2): 6-9 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kumar M, C S J, K P A. A morphological study with clinical, pathological, and immunohistochemical characterization of non-Hodgkin lymphoma. mljgoums 2025; 19 (2) :6-9
URL: http://mlj.goums.ac.ir/article-1-1540-en.html
URL: http://mlj.goums.ac.ir/article-1-1540-en.html



1- Department of Pathology, Father Muller Medical College, Rajiv Gandhi University of Health Sciences, Karnataka, India , mohitchohil@gmail.com
2- Department of Pathology, Father Muller Medical College, Rajiv Gandhi University of Health Sciences, Karnataka, India
2- Department of Pathology, Father Muller Medical College, Rajiv Gandhi University of Health Sciences, Karnataka, India
Full-Text [PDF 535 kb]
(348 Downloads)
| Abstract (HTML) (1048 Views)
Most lesions were of lymph nodal origin (29/48 = 60.42%). The cervical lymph node group was most frequently affected (17/48 = 35.42%), followed by the axillary group (7/48 = 14.58%) and inguinal group (2/48 = 4.17%). The most common extranodal sites were the retroperitoneum (5/48 = 10.42%) and stomach (4/48 = 8.33%). The frequency of lesional sites is detailed in Table 3.
On histopathological evaluation, non-Hodgkin lymphoma without further subtyping was the most common diagnosis (33/48 = 68.75%). Among cases where subtyping was performed based on histomorphology, follicular lymphoma (3/48 = 6.25%) and diffuse large B-cell lymphoma (DLBCL) (3/48 = 6.25%) were equally common. Diagnostic frequencies are presented in Table 4. Representative histopathological images of DLBCL and follicular lymphoma are shown in Figure 1 and Figure 2, respectively.
Discussion
NHL is more prevalent in developed countries, with the highest incidence rates observed in North America and Australia. Lower incidence rates are documented in South-Central and Eastern Asia.
NHL demonstrates a male predominance globally. The worldwide age-standardized rate (ASR) is 6.1/100,000 in males compared to 4.2/100,000 in females. Our study similarly showed higher male incidence (56%) than female (44%). This gender disparity has been consistently reported by Kalyan et al. and Morton et al. (12,13). Multiple studies confirm that NHL incidence increases with age, peaking during the 5th and 6th decades of life.
Roy et al. reported that 63.6% of NHL cases occurred in patients aged 51-60 years (1). Vallabhajosyula et al. documented a median age of 55.5 years in their study population (14), while Padhi et al. found the highest incidence between the 4th and 5th decades (15).
Sharma et al.'s single-center study of 77 NHL cases revealed that B-cell lymphomas accounted for 89.3% of cases, with T-cell lymphomas comprising 10.7%. Diffuse Large B-Cell Lymphoma (DLBCL) was the most frequent subtype (46.8%), while Follicular Lymphoma (FL) and Mantle Cell Lymphoma (MCL) showed lower prevalence in India compared to Western countries (7). Our findings corroborate DLBCL as the predominant NHL subtype. Comparative data from various studies are presented in Table 6.
Gupta et al.'s immunohistochemical analysis of 100 NHL cases demonstrated distinct subtype distribution patterns in India compared to global trends (3). Borgohain et al., in their 50-patient study, established PAX5 as a reliable pan-B cell marker and CD5 as a pan-T cell marker for resource-limited settings. Their findings confirmed the global increase in NHL incidence, with DLBCL being more prevalent in India compared to FL and MCL (16).
Aggarwal et al.'s study of 52 NHL cases concluded that the REAL classification remains applicable even with basic immunohistochemical panels, facilitating B- and T-cell lymphoma differentiation in centers with limited resources (17). Their findings, along with studies by Naresh et al., El-Esawy et al., and Nair et al., consistently identified DLBCL as the most common NHL subtype (18,19). This pattern was also observed in Mushtaq et al.'s Pakistani study (20).
Conclusion
The global incidence of Non-Hodgkin lymphoma (NHL) demonstrates a consistent upward trend, with India showing particularly high rates. Our study identified Diffuse Large B-Cell Lymphoma (DLBCL) and follicular lymphoma as the predominant NHL subtypes. Immunohistochemistry proved essential for both accurate subclassification of NHL and discrimination between malignant and reactive lymphoid proliferations.
While cervical lymph nodes represented the most frequent site of involvement (35.42%), our findings notably included rare presentations in uncommon anatomical locations such as the testis and parasacral region. This observation underscores the importance of considering NHL in the differential diagnosis of lesions at atypical sites.
Acknowledgement
Not applicable
Funding sources
Not applicable
Ethical statement
Approved by the ethical committee.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
JP helped with IHC interpretations. All authors read and approved the final manuscript.
Data availability statement
It will be accessible with the author listed as the corresponding contact.
Full-Text: (44 Views)
Introduction
Lymphadenopathy is a frequent clinical problem, and biopsies are often used to establish the cause of enlarged lymph nodes. It may be neoplastic or non-neoplastic. The neoplastic conditions are mainly metastases and lymphohematogenous malignancies. The non-neoplastic lymphadenopathy has a diverse etiology and can be caused by infections, drug reactions, and non-neoplastic lymphoproliferative disorders like Castleman disease (1).
Numerous classifications of NHL have been proposed, starting with the first one presented by Gall and Mallory in the early 19th century. In 1982, a working formula (WF) was proposed. This working formula divided NHLs into three histological groups depending on the clinical behavior: low, moderate, and high grade. REAL (Revised European American Lymphoma) classification was proposed in 1994, taking into account various shortcomings of WF. The REAL classification is based on morphology, immunophenotypic and cytogenetic data in lymphoma cases (2).
It is the 11th most common cancer worldwide, with a five-year survival rate of 35 percent.
In terms of incidence, the disease accounts for approximately 5.1% of all cancer cases and 2.7% of all cancer deaths. In India, incidence rates for NHL in men and women are 2.9/100,000 and 1.5/100,000, respectively (3). In India, there are approximately 23,718 new NHL cases reported each year (4).
NHLs are slightly more frequent in developed countries (50.5 % of cases worldwide), with the highest rates in Australia and North America and relatively low rates throughout Asia and Eastern Europe (5). In Asia, the incidence of NHL has increased in recent years. Within India, the incidence is several-fold higher in the urban population compared to the rural population. Hence, urban lifestyles and economic progress may increase cancer incidence (3).
The diagnosis of NHL is usually made on Hematoxylin and Eosin-based morphological examination. Immunohistochemistry can differentiate the lymphocytes into T and B cells (6). Various specimens like lymph nodes, bone marrow aspirates, trephine biopsy cores, peripheral blood, and other fluids such as cerebrospinal fluid (CSF), ascitic fluid, and pleural aspirates can be used for lymphoma diagnosis, depending on the presenting clinical symptoms (3).
Non-Hodgkin lymphoma (NHL) comprises a heterogeneous group of neoplasms arising from different lymphoid cell lineages at various stages of development. Non-Hodgkin Lymphomas have discrete causes and demonstrate unique patterns of behavior and responses to the treatment given (7). It is characterized by the neoplastic proliferation of lymphoid tissue, including lymphocytes, histiocytes, and their precursors (3).
NHL etiology is mainly unknown. Infectious agents, severe immunodeficiency, blood transfusion, pesticides, and solvent contact have been constantly reported with increased NHL risk (8). It generally presents as painless, localized, or generalized lymphadenopathy (9). It may present as an extranodal lesion, too. The gastrointestinal tract is the most common extranodal site for NHL, and the other areas include the testis, bones, eyes, brain, heart, white blood cells, skin, and kidneys (10).
NHL can be subclassified based on the stage of maturation into the immature and mature types of NHL. On the other hand, it can be subclassified based on the cell of origin into B cell, T cell, or natural killer cell [NK cell] type of lymphoma (11).
Immunohistochemistry (IHC) is applied in 3 circumstances: It determines the phenotype of the abnormal population detected by morphology, differentiates an abnormal population recognized by flow cytometry, and screens apparently ‘‘reactive’’ tissue to determine whether a subtle abnormal population is present (11).
The occurrence of NHL is higher in the male population in India and worldwide (4,1). NHL in India has a median age of 54 years, a higher male-to-female ratio, a higher proportion of patients with B-symptoms, higher frequency of diffuse large B-cell lymphomas (11).
This study is conducted to assess the clinical presentation of various NHL subtypes, taking IHC as the gold standard, and to study the histo-morphological subtypes of NHL with immunohistochemical correlation.
Methods
This retrospective study was conducted on all specimens diagnosed as NHL by immunohistochemical staining in the pathology department, Father Muller Medical College, Mangalore, Karnataka, India, for 24 months, from March 2018 to February 2020. Institutional ethical clearance was obtained (FMrEC/CCM /s3e/2020). The specimens were fixed in 10 % formalin, and representative sections were obtained. Clinical details such as age, gender, site of the lesion, and Nodal / extranodal presentation are recorded. Histopathological analysis was performed, and Immunohistochemical reports were obtained. Further histopathological findings were correlated with IHC results. Statistical analysis was done based on frequency.
Results
This study included a total of 48 cases. The majority of cases were in the age range of 61 to 70 years (14/48 = 29.17%), followed by 51 to 60 years (9/48 = 18.75%). Five cases (10.42%) were below 20 years of age. The age range and frequency distribution are presented in Table 1. Male predominance was observed (27/48 = 56.25%).
Lymphadenopathy is a frequent clinical problem, and biopsies are often used to establish the cause of enlarged lymph nodes. It may be neoplastic or non-neoplastic. The neoplastic conditions are mainly metastases and lymphohematogenous malignancies. The non-neoplastic lymphadenopathy has a diverse etiology and can be caused by infections, drug reactions, and non-neoplastic lymphoproliferative disorders like Castleman disease (1).
Numerous classifications of NHL have been proposed, starting with the first one presented by Gall and Mallory in the early 19th century. In 1982, a working formula (WF) was proposed. This working formula divided NHLs into three histological groups depending on the clinical behavior: low, moderate, and high grade. REAL (Revised European American Lymphoma) classification was proposed in 1994, taking into account various shortcomings of WF. The REAL classification is based on morphology, immunophenotypic and cytogenetic data in lymphoma cases (2).
It is the 11th most common cancer worldwide, with a five-year survival rate of 35 percent.
In terms of incidence, the disease accounts for approximately 5.1% of all cancer cases and 2.7% of all cancer deaths. In India, incidence rates for NHL in men and women are 2.9/100,000 and 1.5/100,000, respectively (3). In India, there are approximately 23,718 new NHL cases reported each year (4).
NHLs are slightly more frequent in developed countries (50.5 % of cases worldwide), with the highest rates in Australia and North America and relatively low rates throughout Asia and Eastern Europe (5). In Asia, the incidence of NHL has increased in recent years. Within India, the incidence is several-fold higher in the urban population compared to the rural population. Hence, urban lifestyles and economic progress may increase cancer incidence (3).
The diagnosis of NHL is usually made on Hematoxylin and Eosin-based morphological examination. Immunohistochemistry can differentiate the lymphocytes into T and B cells (6). Various specimens like lymph nodes, bone marrow aspirates, trephine biopsy cores, peripheral blood, and other fluids such as cerebrospinal fluid (CSF), ascitic fluid, and pleural aspirates can be used for lymphoma diagnosis, depending on the presenting clinical symptoms (3).
Non-Hodgkin lymphoma (NHL) comprises a heterogeneous group of neoplasms arising from different lymphoid cell lineages at various stages of development. Non-Hodgkin Lymphomas have discrete causes and demonstrate unique patterns of behavior and responses to the treatment given (7). It is characterized by the neoplastic proliferation of lymphoid tissue, including lymphocytes, histiocytes, and their precursors (3).
NHL etiology is mainly unknown. Infectious agents, severe immunodeficiency, blood transfusion, pesticides, and solvent contact have been constantly reported with increased NHL risk (8). It generally presents as painless, localized, or generalized lymphadenopathy (9). It may present as an extranodal lesion, too. The gastrointestinal tract is the most common extranodal site for NHL, and the other areas include the testis, bones, eyes, brain, heart, white blood cells, skin, and kidneys (10).
NHL can be subclassified based on the stage of maturation into the immature and mature types of NHL. On the other hand, it can be subclassified based on the cell of origin into B cell, T cell, or natural killer cell [NK cell] type of lymphoma (11).
Immunohistochemistry (IHC) is applied in 3 circumstances: It determines the phenotype of the abnormal population detected by morphology, differentiates an abnormal population recognized by flow cytometry, and screens apparently ‘‘reactive’’ tissue to determine whether a subtle abnormal population is present (11).
The occurrence of NHL is higher in the male population in India and worldwide (4,1). NHL in India has a median age of 54 years, a higher male-to-female ratio, a higher proportion of patients with B-symptoms, higher frequency of diffuse large B-cell lymphomas (11).
This study is conducted to assess the clinical presentation of various NHL subtypes, taking IHC as the gold standard, and to study the histo-morphological subtypes of NHL with immunohistochemical correlation.
Methods
This retrospective study was conducted on all specimens diagnosed as NHL by immunohistochemical staining in the pathology department, Father Muller Medical College, Mangalore, Karnataka, India, for 24 months, from March 2018 to February 2020. Institutional ethical clearance was obtained (FMrEC/CCM /s3e/2020). The specimens were fixed in 10 % formalin, and representative sections were obtained. Clinical details such as age, gender, site of the lesion, and Nodal / extranodal presentation are recorded. Histopathological analysis was performed, and Immunohistochemical reports were obtained. Further histopathological findings were correlated with IHC results. Statistical analysis was done based on frequency.
Results
This study included a total of 48 cases. The majority of cases were in the age range of 61 to 70 years (14/48 = 29.17%), followed by 51 to 60 years (9/48 = 18.75%). Five cases (10.42%) were below 20 years of age. The age range and frequency distribution are presented in Table 1. Male predominance was observed (27/48 = 56.25%).
|
Table 1.Distribution frequency of age range
 |
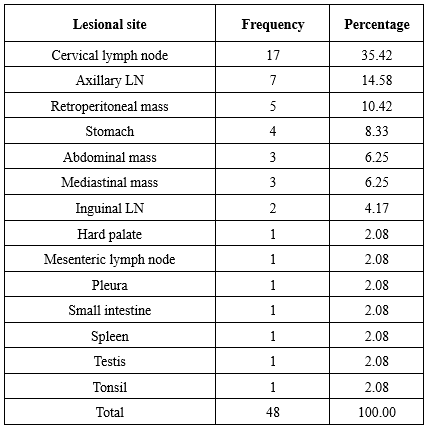
Most lesions were of lymph nodal origin (29/48 = 60.42%). The cervical lymph node group was most frequently affected (17/48 = 35.42%), followed by the axillary group (7/48 = 14.58%) and inguinal group (2/48 = 4.17%). The most common extranodal sites were the retroperitoneum (5/48 = 10.42%) and stomach (4/48 = 8.33%). The frequency of lesional sites is detailed in Table 3.
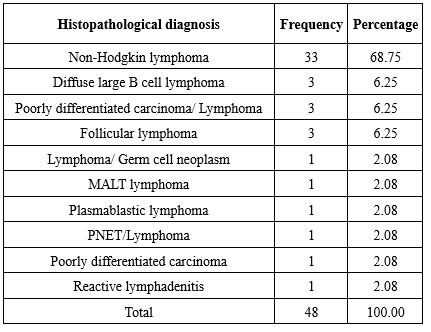
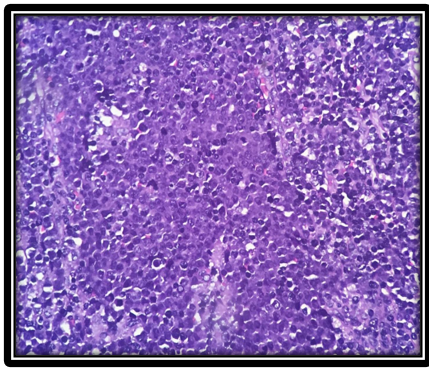
On histopathological evaluation, non-Hodgkin lymphoma without further subtyping was the most common diagnosis (33/48 = 68.75%). Among cases where subtyping was performed based on histomorphology, follicular lymphoma (3/48 = 6.25%) and diffuse large B-cell lymphoma (DLBCL) (3/48 = 6.25%) were equally common. Diagnostic frequencies are presented in Table 4. Representative histopathological images of DLBCL and follicular lymphoma are shown in Figure 1 and Figure 2, respectively.

Immunohistopathological evaluation revealed that B-cell neoplasms (41/48 = 85.42%) were more prevalent than T-cell neoplasms (7/48 = 14.58%). DLBCL was the most common NHL subtype (25/48 = 52.08%), followed by follicular lymphoma (8/48 = 16.67%). Other observed B-cell neoplasms included mantle cell lymphoma, Burkitt lymphoma, high-grade B-cell lymphoma, marginal zone lymphoma, mediastinal large B-cell lymphoma, and plasmablastic lymphoma. Identified T-cell neoplasms comprised angioimmunoblastic T-cell lymphoma, adult T-cell lymphoma, peripheral T-cell lymphoma, precursor T-lymphoblastic lymphoma, and anaplastic large cell lymphoma. The frequency distribution of neoplasms is shown in Table 5.
Comparison between clinical diagnoses and histopathological findings showed correlation in 45 of 48 cases. One clinically suspected gastrointestinal stromal tumor was histopathologically diagnosed as DLBCL. Similarly, a case clinically diagnosed as neuroendocrine tumor of the small intestine and another as epidural abscess were histopathologically identified as DLBCL and peripheral neuroendocrine tumor (PNET)/lymphoma, respectively. Immunohistochemistry confirmed DLBCL in one clinically suspected and histopathologically diagnosed case of reactive lymphadenopathy.
Comparison between clinical diagnoses and histopathological findings showed correlation in 45 of 48 cases. One clinically suspected gastrointestinal stromal tumor was histopathologically diagnosed as DLBCL. Similarly, a case clinically diagnosed as neuroendocrine tumor of the small intestine and another as epidural abscess were histopathologically identified as DLBCL and peripheral neuroendocrine tumor (PNET)/lymphoma, respectively. Immunohistochemistry confirmed DLBCL in one clinically suspected and histopathologically diagnosed case of reactive lymphadenopathy.


Discussion
NHL is more prevalent in developed countries, with the highest incidence rates observed in North America and Australia. Lower incidence rates are documented in South-Central and Eastern Asia.
NHL demonstrates a male predominance globally. The worldwide age-standardized rate (ASR) is 6.1/100,000 in males compared to 4.2/100,000 in females. Our study similarly showed higher male incidence (56%) than female (44%). This gender disparity has been consistently reported by Kalyan et al. and Morton et al. (12,13). Multiple studies confirm that NHL incidence increases with age, peaking during the 5th and 6th decades of life.
Roy et al. reported that 63.6% of NHL cases occurred in patients aged 51-60 years (1). Vallabhajosyula et al. documented a median age of 55.5 years in their study population (14), while Padhi et al. found the highest incidence between the 4th and 5th decades (15).
Sharma et al.'s single-center study of 77 NHL cases revealed that B-cell lymphomas accounted for 89.3% of cases, with T-cell lymphomas comprising 10.7%. Diffuse Large B-Cell Lymphoma (DLBCL) was the most frequent subtype (46.8%), while Follicular Lymphoma (FL) and Mantle Cell Lymphoma (MCL) showed lower prevalence in India compared to Western countries (7). Our findings corroborate DLBCL as the predominant NHL subtype. Comparative data from various studies are presented in Table 6.
Gupta et al.'s immunohistochemical analysis of 100 NHL cases demonstrated distinct subtype distribution patterns in India compared to global trends (3). Borgohain et al., in their 50-patient study, established PAX5 as a reliable pan-B cell marker and CD5 as a pan-T cell marker for resource-limited settings. Their findings confirmed the global increase in NHL incidence, with DLBCL being more prevalent in India compared to FL and MCL (16).
Aggarwal et al.'s study of 52 NHL cases concluded that the REAL classification remains applicable even with basic immunohistochemical panels, facilitating B- and T-cell lymphoma differentiation in centers with limited resources (17). Their findings, along with studies by Naresh et al., El-Esawy et al., and Nair et al., consistently identified DLBCL as the most common NHL subtype (18,19). This pattern was also observed in Mushtaq et al.'s Pakistani study (20).
|
Table 6. Comparison with various other studies
 |
Conclusion
The global incidence of Non-Hodgkin lymphoma (NHL) demonstrates a consistent upward trend, with India showing particularly high rates. Our study identified Diffuse Large B-Cell Lymphoma (DLBCL) and follicular lymphoma as the predominant NHL subtypes. Immunohistochemistry proved essential for both accurate subclassification of NHL and discrimination between malignant and reactive lymphoid proliferations.
While cervical lymph nodes represented the most frequent site of involvement (35.42%), our findings notably included rare presentations in uncommon anatomical locations such as the testis and parasacral region. This observation underscores the importance of considering NHL in the differential diagnosis of lesions at atypical sites.
Acknowledgement
Not applicable
Funding sources
Not applicable
Ethical statement
Approved by the ethical committee.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
JP helped with IHC interpretations. All authors read and approved the final manuscript.
Data availability statement
It will be accessible with the author listed as the corresponding contact.
Research Article: Original Paper |
Subject:
Pathology
Received: 2023/03/30 | Accepted: 2023/05/22 | Published: 2025/07/28 | ePublished: 2025/07/28
Received: 2023/03/30 | Accepted: 2023/05/22 | Published: 2025/07/28 | ePublished: 2025/07/28
References
1. Roy A, Kar R, Basu D, Badhe BA. The spectrum of histopathologic diagnosis of lymph node biopsies: A descriptive study from a tertiary care center in South India over 5½ years. Indian Journal of Pathology and Microbiology. 2013; 56(2): 103. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Harris NL, JaffesES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A revised European American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group. Blood. 1994; 84: 1361-92 [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Gupta V, Singh S, Bhatia Y. Non-Hodgkin's lymphoma: an immunohistochemical analysis with clinicopathological correlation. International Journal of Current Research. 2018; 10(08): 72350-55. [View at Publisher]
4. Yeole BB. Trends in the incidence of Non-Hodgkin's lymphoma in India. Asian Pac J Cancer Prev. 2008; 9(3): 433-6. [View at Publisher] [PMID] [Google Scholar]
5. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin,2005; 55(2):74-108. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Krenacs L, Bagdi E, Krenacs T. Bancroft Theory and Practice of Histological Techniques. 5th ed. Nottingham. Immunocytopathology of Lymphomas; 517-35
7. Sharma M, Mannan R, Madhukar M, Navani S, Manjari M, Bhasin TS, et al . Immunohistochemical (IHC) Analysis of Non-Hodgkin's Lymphoma (NHL) Spectrum According to WHO/REAL Classification: A Single Centre Experience from Punjab, India. Journal of clinical and diagnostic research. 2014; 8(1): 46-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Altieri A, Bermejo JL, Hemminki K. Familial risk for non-Hodgkin lymphoma and other lymphoproliferative malignancies by histopathologic subtype: the Swedish Family-Cancer Database. Blood. 2005; 106(2): 668-72 [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Chang KL, Arber DA, Weiss LM. Lymph nodes and spleen. In: Wick MR, Livolsi VA, Pfeifer JD, Stelow EB, Wakely PE, (eds.) Silverberg's Principles and Practice of Surgical Pathology and Cytopathology. 5th ed. Philedelphia, PA: Elsevier Churchill Livingstone,2015.719- 60.
10. Akhter A, Rahman MR, Majid N, Shermin S, Saleheen MS, Rajib RC, et al. Histological Subtypes of Non-Hodgkin's Lymphoma in Different Age and Sex Groups. Bangladesh Med J. 2012; 41(1):32-6 [DOI] [Google Scholar]
11. Higgins RA, Blankenship JE, Kinney MC. Application of immunohistochemistry in the diagnosis of non-Hodgkin and Hodgkin lymphoma. Archives of pathology & laboratory medicine. 2008; 132(3): 441-61. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Kalyan K, Basu D, Soundararaghavan J. Immunohistochemical typing of nonHodgkin's lymphoma-comparing working formulation and WHO classification. Indian J PatholMicrobiol. 2006; 49(2): 203-7. [View at Publisher] [PMID] [Google Scholar]
13. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992- 2001. Blood. 2006; 107(1): 265-76. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Vallabhajosyula S, Baijal G, Vadhiraja B M, Fernandes DJ, Vidyasagar M S. NonHodgkin's lymphoma: Is India ready to incorporate recent advances in day-to-day practice? J Can Res Ther. 2010; 6: 36-40. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Padhi S, Paul TR, Challa S, Prayaga AK, Rajappa S, Raghunadharao D, et al. Primary Extra Nodal Non-Hodgkin Lymphoma: A 5 Year Retrospective Analysis. Asian Pacific J Cancer Prev. 2012; 13(10): 4889-95. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Borgohain M, Krishnatreya K, Weingken C, Das J. Diagnostic Utility of Immunohistochemistry in Lymphoma. International Journal of Contemporary Medical Research. 2020; 4(12): 162-64. [View at Publisher] [Google Scholar]
17. Aggarwal D, Gupta R, Singh S, Kudesia M. Comparison of working formulation and REAL classification of non-Hodgkin's lymphoma: an analysis of 52 cases. Hematology. 2011; 16(4): 195-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Naresh KN, Srinivas V, Soman CS. Distribution of various subtypes of non-Hodgkin's lymphoma in India: a study of 2773 lymphomas using R.E.A.L. and WHO Classifications. Ann Oncol. 2000; 11(1): 63-7 [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Nair R, Arora N, Mallath MK. Epidemiology of NonHodgkin's Lymphoma in India. Oncology. 2016; 91(1):18-25. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Mushtaq S, Akhtar N, Jamal S, Mamoon N, Khadim T, Sarfaraz T, et al. Malignant lymphomas in Pakistan according to the WHO classification of lymphoid neoplasms. Asian Pac J Cancer Prev. 2008; 9(2): 229-32. [View at Publisher] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.