
Fri, Oct 3, 2025
Volume 18, Issue 1 (Jan-Feb 2024)
mljgoums 2024, 18(1): 1-3 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bhide S, Lahane R. Histopathological spectrum of upper gastrointestinal endoscopic biopsies in a rural teaching hospital. mljgoums 2024; 18 (1) :1-3
URL: http://mlj.goums.ac.ir/article-1-1592-en.html
URL: http://mlj.goums.ac.ir/article-1-1592-en.html



1- Department of Pathology, MIMER Medical College Talegaon Dabhade Maharashtra Pune India- MAEER MIT Pune's MIMER Medical College & Dr. BSTR Hospital Talegaon Dabhade Pune, India , smitapbhide@yahoo.co.in
2- Department of Pathology, SRTR Medical College Ambejogai Maharashtra India- SRTR Medical College Ambejogai, India
2- Department of Pathology, SRTR Medical College Ambejogai Maharashtra India- SRTR Medical College Ambejogai, India
Keywords: Endoscopic Biopsy (Endoscopic Mucosal Resection), Histopathological Spectrum, Upper Gastrointestinal Tract, Endoscopic Mucosal Resection, Hospitals, Teaching
Full-Text [PDF 434 kb]
(894 Downloads)
| Abstract (HTML) (4306 Views)
Full-Text: (1009 Views)
Introduction
The upper gastrointestinal (GI) tract consists of the oral cavity, salivary glands, esophagus, stomach, and small intestine (duodenum, jejunum, and ileum) (1). Disorders affecting the upper GI tract often present with a similar group of symptoms, making clinical assessment challenging (2,3). Upper GI endoscopy, which provides visualization of the upper GI tract up to the duodenum, is an established diagnostic and therapeutic procedure for a wide range of upper GI conditions. It also allows for the biopsy of both neoplastic and non-neoplastic lesions. This procedure is simple, safe, well-tolerated, and offers direct visualization of the pathological site, enabling early detection of pathological changes and facilitating the initiation of appropriate treatment (3).
Endoscopic biopsy examination, followed by histopathological assessment, is a convenient and currently accepted gold standard for accurately and objectively evaluating patients with upper GI symptoms (4,5).
Upper gastrointestinal tract (GIT) disorders are among the most frequently encountered issues in clinical practice, often associated with significant morbidity and mortality. Endoscopic biopsy is a common procedure performed in hospitals to investigate a variety of benign and malignant lesions. Evaluating the upper GIT can provide critical information that informs decisions about future surgical interventions. Consequently, having a comprehensive understanding of the spectrum of lesions that can be diagnosed in these specimens is essential for making accurate diagnoses and improving patient management (6-11).
Therefore, the present study was conducted at our tertiary care center to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings. Additionally, we aimed to determine the frequency of occurrence of these lesions in relation to age and sex.
Methods
The present study was conducted at our tertiary care center and involved the examination of 70 patients to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings. The study also aimed to determine the frequency of occurrence of these lesions with respect to age and sex.
This prospective study spanned a period of 2 years and included 70 patients.
Inclusion Criteria: The study encompassed all endoscopic biopsies of the upper
GIT received in the Department of Pathology.
Exclusion Criteria: Biopsies of the oral cavity and pharynx, as well as biopsies beyond the second part of the duodenum, were excluded from the study.
Methodology: Following approval from the Institutional Ethics Committee (Reference No. IEC 531 dated 10/10/2018), valid informed consent was obtained
from all participants. Once enrolled, patients underwent a thorough history and physical examination according to a predefined form. Relevant patient information, including age, registration number, presenting signs and symptoms, as well as past medical history and endoscopic findings, were recorded. The collected biopsies were placed in properly labeled and tightly sealed containers containing 10% formalin. These specimens were grossly examined to assess their number and appearance. After adequate fixation, the entire biopsy was processed routinely and embedded in paraffin with the mucosal surface positioned uppermost. Thin sections, approximately 4-5 microns thick, were cut perpendicular to this surface using a rotary microtome, with 3-4 serial sections prepared on each slide. Subsequently, these sections were stained with hematoxylin and eosin (H&E). Special stains, such as Giemsa, were applied when necessary. The histopathological classification of tumors followed the recommendations of the World Health Organization (WHO).
Results
The present study is a prospective analysis of 70 consecutive upper GI endoscopic biopsies received in the Department of Pathology at our college. It aimed to determine the spectrum of upper GI lesions through endoscopic biopsies. Below are the results of the analysis of these seventy cases.
Out of the 70 upper GI endoscopic biopsy samples studied during the period, 25 (35.71%) were from the esophagus, 35 (50.0%) from the stomach, and 10 (14.29%) from the duodenum.
The highest number of biopsies were performed on patients between 51 and 60 years and 61 to 70 years (21.4%), followed by 41 to 50 years (15.7%). The lowest incidence was observed in the age group of 11-20 years (1.7%), followed by 31 to 40 years (11.8%). Among the patients, there were 47 males and 23 females, resulting in a male-to-female ratio of 2.1:1.
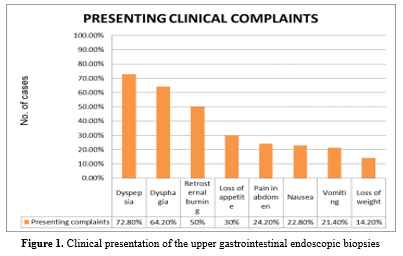
Among the patients, 72.80% presented with dyspepsia, while 64.20% reported dysphagia. Other chief complaints included abdominal pain, retrosternal burning, vomiting, loss of appetite, weight loss, and nausea. (Figure1)
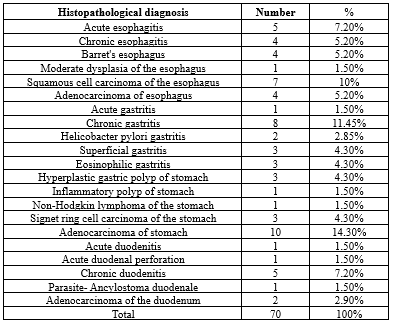
Upon histopathological examination of endoscopic biopsies from the upper GIT, it was observed that inflammatory lesions were the most common (48.57%), followed by malignant lesions (38.58%). Benign lesions accounted for 12.85% of the cases. (Table1)
Result shows that non-neoplastic lesions accounted for 48.57% of all upper GI biopsies in the present study. Gastric lesions (24.28%) were the most commonly found, followed by esophageal lesions (12.85%) and duodenal lesions (11.42%). The most commonly encountered non-neoplastic lesions were esophagitis, chronic gastritis, and chronic duodenitis.
Premalignant lesions accounted for 7.20% of all biopsies and were primarily observed in the esophagus. Dysplasia in the esophagus accounted for 1.50% of all biopsies, while dysplasia was not seen in biopsies from the stomach and duodenum. Barrett's esophagus (Figure 2a) was seen in 5.20% of all esophageal biopsies.
In terms of neoplastic lesions in the upper gastrointestinal (GI) tract, the study identified four cases (5.20%) of benign polyps, comprising three hyperplastic gastric polyps and one inflammatory polyp.
A total of 27 cases (38.57%) of upper GI malignancies were identified, with 15.71% in the esophagus (Figure 2b), 20% in the stomach, and 2.85% in the duodenum. Male predominance was observed in all malignancies. (Table 1)
Out of 32 patients suspected of having malignancy on endoscopy, 27 (38.57%) of them showed malignancy on histopathology. The remaining 5 cases (7.14%) were benign on histopathology. Among the 10 (14.28%) patients suspected of having benign lesions on endoscopy, 9 cases (12.85%) turned out to be benign, while 1 (1.42%) was malignant histopathologically. Twenty-eight (40%) patients had different endoscopic findings, such as ulceration, hyperemia, reddish mucosa, and whitish worms. These were non-neoplastic lesions histopathologically.

Discussion
The present study was conducted at our tertiary care center on 70 patients to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings, as well as to determine their frequency of occurrence based on age and sex.
In the present study, the most common site for biopsy was the stomach (50%), followed by the esophagus (35%) and duodenum (15%). This finding aligns with the studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Rashmi K et al. (3), Sharma et al. (16), Aparajita A et al. (17), Bhat N et al. (18), Syed Imtiyaz Hussain et al. (19), and Veenaa Venkatesh et al. (20).
In our study, most of the cases were between 50-70 years of age. This finding is consistent with the studies conducted by Jaynul Islam SK et al. (12), Somani NS et al. (14), Aparajita A et al. (17), Siddiqui et al. (21), Syed Imtiyaz Hussain et al. (19), and Mittal T et al. (22).
In the present study, a male preponderance was observed, with a male-to-female ratio of 2.1:1. This finding is in line with the studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Rashmi K et al. (3), Sharma et al. (16), Patil AS et al. (23), Aparajita A et al. (17), Bhat N et al. (18), Siddiqui et al. (21), Sahu PR et al. (24), Puturaju S et al. (25), Syed Imtiyaz Hussain et al. (19), Mittal T et al. (22), Thapa R et al. (26), and Veenaa Venkatesh et al. (20).
The most common clinical symptom in the present study was dyspepsia (72.85%), followed by dysphagia (64.8%). This finding is consistent with the studies conducted by Somani NS et al. (14), Mohan B et al. (15), Qureshi N A et al. (27), and Syed Imtiyaz Hussain et al. (19).
In the present study, the most common non-neoplastic esophageal lesion was esophagitis (12.40%), followed by a neoplastic lesion, squamous cell carcinoma (10.0%). These findings align with studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Rashmi K et al. (3), Qureshi N A et al. (27), and Sharma S et al. (28).
The most common site for esophageal malignancy in the present study was the middle one-third (32.0%) of the esophagus. Squamous cell carcinoma (10%) was the predominant lesion, while adenocarcinoma was seen in 5.20% of cases. These findings were consistent with studies done by Jaynul Islam SK et al. (12), Mohan B et al. (15), Rashmi K et al. (3), Somani NS et al. (14), and Ganga H et al. (13), where squamous cell carcinoma was the most common malignancy, occurring predominantly in the middle third of the esophagus.
In the present study, the most common lesions found in the stomach were inflammatory (48.5%), followed by malignant lesions (40%), while benign lesions constituted 11.5%. The most common non-neoplastic lesion was chronic gastritis (28.58%), and 2.85% of cases showed Helicobacter pylori-associated gastritis. The most common malignant lesion in gastric biopsies was adenocarcinoma (28.58%), followed by signet-ring cell carcinoma (8.58%). Endoscopically, malignant lesions showed predominantly ulcerative proliferative growth and polypoidal growth. These findings are consistent with studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Qureshi N A et al. (27), Sharma S et al. (28), Rashmi K et al. (3), and Shilpi Sahu et al. (29).
In the present study, the most common lesions found in the duodenum were chronic duodenitis (50%) and adenocarcinoma (20%). These findings are consistent with studies conducted by Mohan B et al. (15) and Veenaa Venkatesh et al. (20).
Out of all biopsies done in the present study, the most common malignancies observed were from the stomach (20.10%), followed by the esophagus (15.20%) and duodenum (2.90%). This is comparable to findings in studies by Somani NS et al. (14), Veenaa Venkatesh et al. (20), and Syed Imtiyaz Hussain et al. (19).
Conclusion
Biopsy sampling of the upper GI mucosa during diagnostic endoscopy provides valuable information. Endoscopy, when combined with biopsy, becomes a powerful diagnostic tool that significantly contributes to improved patient management. Histopathology is considered the gold standard for diagnosing lesions detected through endoscopy. Biopsy offers an excellent opportunity for clinicians and histopathologists to correlate clinical data, endoscopic findings, and pathological lesions.
The present study underscores the importance of upper GI endoscopic biopsy in early detection of malignant lesions, screening for premalignant lesions, and differentiation between non-neoplastic and neoplastic lesions. This, in turn, aids in appropriate patient management.
In conclusion, fiberoptic diagnostic upper GI endoscopy is a relatively less invasive, simple, safe, and well-tolerated procedure. It is cost-effective and provides a high diagnostic yield for confirming various upper GI lesions. In routine clinical practice, histopathology remains the gold standard for definitively diagnosing a wide range of lesions.
Acknowledgement
Not Applicable
Funding sources
Upper GI endoscopic biopsies are routinely performed for diagnosing and managing patients who present with complaints such as dyspepsia, dysphagia, nausea, vomiting, and retrosternal burning. All the necessary instruments were available in the hospital's histopathology laboratory, and no additional funding was required for this study.
Ethical statement
Approval was obtained from the Institutional Ethics Committee (Reference No. IEC 531, dated 10/10/2018), and valid informed consent was obtained from each patient to participate in the study.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
RL collected, analyzed, and interpreted the patient data regarding clinical, endoscopic, and histopathological findings of upper GI endoscopic biopsies. SB performed the histological examination of the upper GI endoscopic biopsies and was a major contributor to writing the manuscript. Both authors have read and approved the final manuscript.
The upper gastrointestinal (GI) tract consists of the oral cavity, salivary glands, esophagus, stomach, and small intestine (duodenum, jejunum, and ileum) (1). Disorders affecting the upper GI tract often present with a similar group of symptoms, making clinical assessment challenging (2,3). Upper GI endoscopy, which provides visualization of the upper GI tract up to the duodenum, is an established diagnostic and therapeutic procedure for a wide range of upper GI conditions. It also allows for the biopsy of both neoplastic and non-neoplastic lesions. This procedure is simple, safe, well-tolerated, and offers direct visualization of the pathological site, enabling early detection of pathological changes and facilitating the initiation of appropriate treatment (3).
Endoscopic biopsy examination, followed by histopathological assessment, is a convenient and currently accepted gold standard for accurately and objectively evaluating patients with upper GI symptoms (4,5).
Upper gastrointestinal tract (GIT) disorders are among the most frequently encountered issues in clinical practice, often associated with significant morbidity and mortality. Endoscopic biopsy is a common procedure performed in hospitals to investigate a variety of benign and malignant lesions. Evaluating the upper GIT can provide critical information that informs decisions about future surgical interventions. Consequently, having a comprehensive understanding of the spectrum of lesions that can be diagnosed in these specimens is essential for making accurate diagnoses and improving patient management (6-11).
Therefore, the present study was conducted at our tertiary care center to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings. Additionally, we aimed to determine the frequency of occurrence of these lesions in relation to age and sex.
Methods
The present study was conducted at our tertiary care center and involved the examination of 70 patients to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings. The study also aimed to determine the frequency of occurrence of these lesions with respect to age and sex.
This prospective study spanned a period of 2 years and included 70 patients.
Inclusion Criteria: The study encompassed all endoscopic biopsies of the upper
GIT received in the Department of Pathology.
Exclusion Criteria: Biopsies of the oral cavity and pharynx, as well as biopsies beyond the second part of the duodenum, were excluded from the study.
Methodology: Following approval from the Institutional Ethics Committee (Reference No. IEC 531 dated 10/10/2018), valid informed consent was obtained
from all participants. Once enrolled, patients underwent a thorough history and physical examination according to a predefined form. Relevant patient information, including age, registration number, presenting signs and symptoms, as well as past medical history and endoscopic findings, were recorded. The collected biopsies were placed in properly labeled and tightly sealed containers containing 10% formalin. These specimens were grossly examined to assess their number and appearance. After adequate fixation, the entire biopsy was processed routinely and embedded in paraffin with the mucosal surface positioned uppermost. Thin sections, approximately 4-5 microns thick, were cut perpendicular to this surface using a rotary microtome, with 3-4 serial sections prepared on each slide. Subsequently, these sections were stained with hematoxylin and eosin (H&E). Special stains, such as Giemsa, were applied when necessary. The histopathological classification of tumors followed the recommendations of the World Health Organization (WHO).
Results
The present study is a prospective analysis of 70 consecutive upper GI endoscopic biopsies received in the Department of Pathology at our college. It aimed to determine the spectrum of upper GI lesions through endoscopic biopsies. Below are the results of the analysis of these seventy cases.
Out of the 70 upper GI endoscopic biopsy samples studied during the period, 25 (35.71%) were from the esophagus, 35 (50.0%) from the stomach, and 10 (14.29%) from the duodenum.
The highest number of biopsies were performed on patients between 51 and 60 years and 61 to 70 years (21.4%), followed by 41 to 50 years (15.7%). The lowest incidence was observed in the age group of 11-20 years (1.7%), followed by 31 to 40 years (11.8%). Among the patients, there were 47 males and 23 females, resulting in a male-to-female ratio of 2.1:1.
Among the patients, 72.80% presented with dyspepsia, while 64.20% reported dysphagia. Other chief complaints included abdominal pain, retrosternal burning, vomiting, loss of appetite, weight loss, and nausea. (Figure1)
Upon histopathological examination of endoscopic biopsies from the upper GIT, it was observed that inflammatory lesions were the most common (48.57%), followed by malignant lesions (38.58%). Benign lesions accounted for 12.85% of the cases. (Table1)
Result shows that non-neoplastic lesions accounted for 48.57% of all upper GI biopsies in the present study. Gastric lesions (24.28%) were the most commonly found, followed by esophageal lesions (12.85%) and duodenal lesions (11.42%). The most commonly encountered non-neoplastic lesions were esophagitis, chronic gastritis, and chronic duodenitis.
Premalignant lesions accounted for 7.20% of all biopsies and were primarily observed in the esophagus. Dysplasia in the esophagus accounted for 1.50% of all biopsies, while dysplasia was not seen in biopsies from the stomach and duodenum. Barrett's esophagus (Figure 2a) was seen in 5.20% of all esophageal biopsies.
In terms of neoplastic lesions in the upper gastrointestinal (GI) tract, the study identified four cases (5.20%) of benign polyps, comprising three hyperplastic gastric polyps and one inflammatory polyp.
A total of 27 cases (38.57%) of upper GI malignancies were identified, with 15.71% in the esophagus (Figure 2b), 20% in the stomach, and 2.85% in the duodenum. Male predominance was observed in all malignancies. (Table 1)
Out of 32 patients suspected of having malignancy on endoscopy, 27 (38.57%) of them showed malignancy on histopathology. The remaining 5 cases (7.14%) were benign on histopathology. Among the 10 (14.28%) patients suspected of having benign lesions on endoscopy, 9 cases (12.85%) turned out to be benign, while 1 (1.42%) was malignant histopathologically. Twenty-eight (40%) patients had different endoscopic findings, such as ulceration, hyperemia, reddish mucosa, and whitish worms. These were non-neoplastic lesions histopathologically.
|
Table 1. The incidence of Upper Gastrointestinal Lesions in the present study
 |
Discussion
The present study was conducted at our tertiary care center on 70 patients to assess the histopathological spectrum of various upper GIT lesions in relation to clinical and endoscopic findings, as well as to determine their frequency of occurrence based on age and sex.
In the present study, the most common site for biopsy was the stomach (50%), followed by the esophagus (35%) and duodenum (15%). This finding aligns with the studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Rashmi K et al. (3), Sharma et al. (16), Aparajita A et al. (17), Bhat N et al. (18), Syed Imtiyaz Hussain et al. (19), and Veenaa Venkatesh et al. (20).
In our study, most of the cases were between 50-70 years of age. This finding is consistent with the studies conducted by Jaynul Islam SK et al. (12), Somani NS et al. (14), Aparajita A et al. (17), Siddiqui et al. (21), Syed Imtiyaz Hussain et al. (19), and Mittal T et al. (22).
In the present study, a male preponderance was observed, with a male-to-female ratio of 2.1:1. This finding is in line with the studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Rashmi K et al. (3), Sharma et al. (16), Patil AS et al. (23), Aparajita A et al. (17), Bhat N et al. (18), Siddiqui et al. (21), Sahu PR et al. (24), Puturaju S et al. (25), Syed Imtiyaz Hussain et al. (19), Mittal T et al. (22), Thapa R et al. (26), and Veenaa Venkatesh et al. (20).
The most common clinical symptom in the present study was dyspepsia (72.85%), followed by dysphagia (64.8%). This finding is consistent with the studies conducted by Somani NS et al. (14), Mohan B et al. (15), Qureshi N A et al. (27), and Syed Imtiyaz Hussain et al. (19).
In the present study, the most common non-neoplastic esophageal lesion was esophagitis (12.40%), followed by a neoplastic lesion, squamous cell carcinoma (10.0%). These findings align with studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Rashmi K et al. (3), Qureshi N A et al. (27), and Sharma S et al. (28).
The most common site for esophageal malignancy in the present study was the middle one-third (32.0%) of the esophagus. Squamous cell carcinoma (10%) was the predominant lesion, while adenocarcinoma was seen in 5.20% of cases. These findings were consistent with studies done by Jaynul Islam SK et al. (12), Mohan B et al. (15), Rashmi K et al. (3), Somani NS et al. (14), and Ganga H et al. (13), where squamous cell carcinoma was the most common malignancy, occurring predominantly in the middle third of the esophagus.
In the present study, the most common lesions found in the stomach were inflammatory (48.5%), followed by malignant lesions (40%), while benign lesions constituted 11.5%. The most common non-neoplastic lesion was chronic gastritis (28.58%), and 2.85% of cases showed Helicobacter pylori-associated gastritis. The most common malignant lesion in gastric biopsies was adenocarcinoma (28.58%), followed by signet-ring cell carcinoma (8.58%). Endoscopically, malignant lesions showed predominantly ulcerative proliferative growth and polypoidal growth. These findings are consistent with studies conducted by Jaynul Islam SK et al. (12), Ganga H et al. (13), Somani NS et al. (14), Mohan B et al. (15), Qureshi N A et al. (27), Sharma S et al. (28), Rashmi K et al. (3), and Shilpi Sahu et al. (29).
In the present study, the most common lesions found in the duodenum were chronic duodenitis (50%) and adenocarcinoma (20%). These findings are consistent with studies conducted by Mohan B et al. (15) and Veenaa Venkatesh et al. (20).
Out of all biopsies done in the present study, the most common malignancies observed were from the stomach (20.10%), followed by the esophagus (15.20%) and duodenum (2.90%). This is comparable to findings in studies by Somani NS et al. (14), Veenaa Venkatesh et al. (20), and Syed Imtiyaz Hussain et al. (19).
Conclusion
Biopsy sampling of the upper GI mucosa during diagnostic endoscopy provides valuable information. Endoscopy, when combined with biopsy, becomes a powerful diagnostic tool that significantly contributes to improved patient management. Histopathology is considered the gold standard for diagnosing lesions detected through endoscopy. Biopsy offers an excellent opportunity for clinicians and histopathologists to correlate clinical data, endoscopic findings, and pathological lesions.
The present study underscores the importance of upper GI endoscopic biopsy in early detection of malignant lesions, screening for premalignant lesions, and differentiation between non-neoplastic and neoplastic lesions. This, in turn, aids in appropriate patient management.
In conclusion, fiberoptic diagnostic upper GI endoscopy is a relatively less invasive, simple, safe, and well-tolerated procedure. It is cost-effective and provides a high diagnostic yield for confirming various upper GI lesions. In routine clinical practice, histopathology remains the gold standard for definitively diagnosing a wide range of lesions.
Acknowledgement
Not Applicable
Funding sources
Upper GI endoscopic biopsies are routinely performed for diagnosing and managing patients who present with complaints such as dyspepsia, dysphagia, nausea, vomiting, and retrosternal burning. All the necessary instruments were available in the hospital's histopathology laboratory, and no additional funding was required for this study.
Ethical statement
Approval was obtained from the Institutional Ethics Committee (Reference No. IEC 531, dated 10/10/2018), and valid informed consent was obtained from each patient to participate in the study.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
RL collected, analyzed, and interpreted the patient data regarding clinical, endoscopic, and histopathological findings of upper GI endoscopic biopsies. SB performed the histological examination of the upper GI endoscopic biopsies and was a major contributor to writing the manuscript. Both authors have read and approved the final manuscript.
Research Article: Original Paper |
Subject:
Pathology
Received: 2022/11/2 | Accepted: 2023/12/11 | Published: 2024/01/24 | ePublished: 2024/01/24
Received: 2022/11/2 | Accepted: 2023/12/11 | Published: 2024/01/24 | ePublished: 2024/01/24
References
1. Varadarajulu S, Eloubeidi MA, Patel RS. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc. 2005;61(7):804-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. DEF Tweedle. Endoscopic interpretation. Normal and pathologic appearances of the gastrointestinal tract. Michael O. Blackstone. 285 × 220 mm. Pp. 575 + xv. Illustrated in black and white and colour. 1984. New York: Raven Press. 1985;72(4):331. [View at Publisher] [DOI] [Google Scholar]
3. Rashmi K, Horakerappa MS, Karar A, Mangala G. A study on histopathologic spectrum of upper gastrointestinal tract endoscopic biopsies. Int J Medical Res Health Sciences. 2013;2(3):418-424. [View at Publisher] [DOI] [Google Scholar]
4. Shepherd NA, Valori RM. The effective use of gastrointestinal histopathology: guidance for endoscopic biopsy in the gastrointestinal tract. Frontline gastroenterology. 2014;5(2):84-87. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Memon F, Baloch K, Memon AA. Upper gastrointestinal endoscopic biopsy; morphological spectrum of lesions. Professional Med J. 2015;22(12):1574-9. [View at Publisher] [DOI] [Google Scholar]
6. Hirachand S, Sthapit RR, Gurung P et al Histopathological spectrum of upper gastrointestinal endoscopic biopsies. J BP Koirala Inst Health Sci. 2018;1(1):67-74. [View at Publisher] [DOI] [Google Scholar]
7. Khatib WM, Demde RB, Aher VC, Patel PM. Histopathological Spectrum of Non-Malignant Lesions of Gastrointestinal Tract- An Institutional Study. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS). 2016;15(10):113-6. [View at Publisher] [DOI] [Google Scholar]
8. Sarker MR, Farooq S, Uddin KS, Akramul Islam ASM, Ali Z. Pattern of upper git lesions diagnosed by Histopathological examination of endoscopic biopsies in a rural tertiary hospital. KYAMC Journal. 2018:9(1):20-3. [View at Publisher] [DOI] [Google Scholar]
9. Gumber R, Mulay SS. Endoscopic biopsy interpretation of Upper gastrointestinal pathologies. international journal of scientific research. 2016;5(10):20-4. [View at Publisher] [Google Scholar]
10. Padma S, Murugan R. Disease pattern by upper gastrointestinal endoscopy in rural areas of Tiruchirappalli district carried out at CMCH and RC Irungalur, retrospective study and comparative analysis with other contemporary studies in India. International Surgery Journal. 2018;5(3):965-70. [View at Publisher] [DOI] [Google Scholar]
11. Peixoto A, Silva M, Pereira P, Macedo G. Biopsies in gastrointestinal endoscopy: When and how. GE Port J Gastroenterol. 2016;23(1):19-27. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Sk Md. Jaynul Islam, Asm Mostaque Ahmed, Samma Hafiz. Endoscopic and Histologic Diagnosis of Upper Gastrointestinal Lesions, Experience in a Port City of Bangladesh. Chattagram Maa-O- Shishu Hospital Medical College Journal. 2014;13(3):11-4. [View at Publisher] [DOI] [Google Scholar]
13. Ganga H, Indudhara PB. Histopathological spectrum of lesions of upper gastrointestinal tract: A study of endoscopic biopsies. Int J Clin Diagnos Pathol. 2018;1(2):21-5. [View at Publisher] [DOI] [Google Scholar]
14. Somani NS, Patil P. Histopathological Study of The Upper Gastrointestinal Tract Endoscopic Biopsies. Annals of Pathology and Laboratory Medicine. 2018;5(8):A683-8. [View at Publisher] [DOI]
15. Mohan B, Manjunath HK, Geethamani V, Dharani VC, Sushma TA, Akshatha B. Histomorphological Analysis of Upper Gastrointestinal Endoscopic Biopsies: A Retrospective Study of 106 Cases. National Journal of Laboratory Medicine. 2019;8(4):PO04-7. [View at Publisher] [DOI] [Google Scholar]
16. Sharma A, Gupta K. Histopathological Spectrum of Upper Gastrointestinal Tract Endoscopic Biopsies In A Tertiary Care Hospital In Rural Population In North India. Int J Adv Res. 2020;8(04):945-50. [View at Publisher] [DOI] [Google Scholar]
17. Aparajita A, Mohanty RC, Sahu AA, Mohanty R, Satpathy PK, Bhuyan T. Histomorphological study of upper GI endoscopic biopsies. Int J Health Sci Res. 2016;6(12):59-64. [View at Publisher] [Google Scholar]
18. Bhat N, Sheikh BA, Mir JN, Reshi R, Wani LA, et al. (2018) Histopathological Study of Upper Gastrointestinal Endoscopic Biopsies-1 Year Prospective Study. Br Biomed Bull. 2013;6(2):315 [View at Publisher] [Google Scholar]
19. Hussain SI, Reshi R, Akhter G, Beigh A. Clinico histopathological study of upper gastrointestinal tract endoscopic biopsies. Int J Cur Res Rev. 2015;7(16):78-85 [View at Publisher] [Google Scholar]
20. Venkatesh V, Thaj RR. Histopathological Spectrum of Lesions in Gastrointestinal Endoscopic Biopsies: A Retrospective Study in a Tertiary Care Center in India. World Journal of Pathology. 2019;10(8):1-6. [Google Scholar]
21. Siddiqui B, Faridi SH, Shehwar D, Ahmed S, Mazumder MA. A Study of Age-Wise Spectrum of Gastrointestinal Biopsies with Endoscopic Correlation a 5-Year Experience from a Tertiary Health Care Centre in North India. Int J Pathol Clin Res. 2020;6 (2). [View at Publisher] [DOI] [Google Scholar]
22. Mittal T, Niranjan J, Prathima S. Histopathological spectrum of upper gastrointestinal endoscopic biopsies of neoplastic lesions: A retrospective study. IP J Diagn Pathol Oncol. 2020;5(4):410-4. [View at Publisher] [DOI] [Google Scholar]
23. Patil AS, Ramachandran M, Mohan RK, et al. Histopathological evaluation of endoscopic biopsies in patients with lesional gastrointestinal tract disorders. J Evolution Med Dent Sci. 2016;5(1):01-3. [View at Publisher] [DOI] [Google Scholar]
24. Sahu PR, Hiwale KM, Vagha SJ. Study of various gastrointestinal tract lesions by endoscopic biopsies in a tertiary care of center of rural district of, Maharashtra. J Evolution Med Dent Sci. 2021;10(16):1135-9. [View at Publisher] [DOI] [Google Scholar]
25. Puttaraju S, Sreramaseshadri SRM. Study of upper gastrointestinal endoscopy in patients with gastrointestinal symptoms. Int Surg J. 2019;6(10):3595-9. [View at Publisher] [DOI] [Google Scholar]
26. Thapa R, Lakhey M, Yadav PK, Kandel P, Aryal C, Subba K. Histopathological study of endoscopic biopsies. JNMA J Nepal Med Assoc. 2013;52(190):354-6. [View at Publisher] [DOI] [Google Scholar]
27. Qureshi NA, Hallissey MT, Fielding JW. Outcome of index upper gastrointestinal endoscopy in patients presenting with dysphagia in a tertiary care hospital-A 10 years review. BMC Gastroenterol. 2007;7:43. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Sharma S, Agarwal L, Rai NN, Agrawal MM. Histopathological spectrum of upper gastrointestinal lesion detected by endoscopy guided biopsy-A single institute experience. IP Archives of Cytology and Histopathology Research. 2019;4(2):154-8. [View at Publisher] [DOI] [Google Scholar]
29. Sahu S, Suryakant WA, Jaiswal R. Endoscopic biopsies - A boon to diagnose gastrointestinal tract diseases. IAIM. 2019;6(12):47-56. [View at Publisher] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.