
Thu, Jul 24, 2025
Volume 18, Issue 1 (Jan-Feb 2024)
mljgoums 2024, 18(1): 9-11 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jaiswal S, Subedi B, Sapkota A, Sharma P, Timilsina M, Timilsina M et al . Prevalence of helicobacter pylori infection and hygiene practices among people with active gastritis. mljgoums 2024; 18 (1) :9-11
URL: http://mlj.goums.ac.ir/article-1-1668-en.html
URL: http://mlj.goums.ac.ir/article-1-1668-en.html
Prevalence of helicobacter pylori infection and hygiene practices among people with active gastritis
Suresh Jaiswal1 

 , Bijay Subedi2 , Ashmita Sapkota2 , Pushpa Sharma2 , Manisha Timilsina2 , Maheshwor Timilsina2 , Bishnu Raj Tiwari2
, Bijay Subedi2 , Ashmita Sapkota2 , Pushpa Sharma2 , Manisha Timilsina2 , Maheshwor Timilsina2 , Bishnu Raj Tiwari2
, Bijay Subedi2 , Ashmita Sapkota2 , Pushpa Sharma2 , Manisha Timilsina2 , Maheshwor Timilsina2 , Bishnu Raj Tiwari2
1- School of Health & Allied Sciences, Pokhara University, Kaski, Nepal , suuress@gmail.com
2- School of Health & Allied Sciences, Pokhara University, Kaski, Nepal
2- School of Health & Allied Sciences, Pokhara University, Kaski, Nepal
Full-Text [PDF 364 kb]
(693 Downloads)
| Abstract (HTML) (2326 Views)
Full-Text: (666 Views)
Introduction
Helicobacter pylori (H. pylori) is a spiral-shaped microaerophilic gram-negative bacterium (1). It is helix-shaped, which is thought to have evolved to penetrate the mucous lining of the stomach (2). It leads to the development of chronic gastritis, gastric ulcers, duodenal ulcers, and mucosal atrophy. Additionally, Helicobacter pylori is recognized as a class I cancer-causing agent because long-lasting inflammation and atrophy can further lead to malignant transformation (3, 4). At least half the world’s population is infected by this bacterium, making it the most widespread infection in the world, especially in the developing world, where rates are estimated to be around 80% (5).
H. pylori infection is an important global infection with a worldwide prevalence of about 50 % (6, 7). This infection is mostly acquired during childhood through the fecal-oral and oral-oral routes (8, 9). Early infection with this bacterium is usually silent, but symptoms and pathologic changes occur later in life. The clinical conditions and pathologic changes associated with H. pylori infection include gastritis, gastric and duodenal ulcers, gastric cancers, iron deficiency anemia, and idiopathic thrombocytopenic purpura (ITP) (10-13).
H. pylori infection shows a variety of geographic distribution on both local communities and large global scales. These variations are mostly due to socioeconomically driven factors such as sex, age, genetic tendency, ethnicity, level of education, and sanitation, which decide the rate and prevalence of this worldwide infection (14-16).
In developing countries, H. pylori is found to be the most common human infection globally. In developing countries, more than 80% of the population test positive for H. pylori (14,17,18).
The main objective of this study was to determine the H. pylori infection in the population of Lekhnath municipality of Kaski district to assess the risk factors for H. pylori by an extended anamnesis, involving data on sex, age, educational level, smoking, drinking, as well as dietary factors.
Methods
A community-based cross-sectional study was carried out from 2018/5/7 to 2019/03/01 at Pokhara 30, earlier known as Lekhnath. Samples were collected from Khudi, Dhungepatan, and the Powerhouse area of Pokhara-30. Only those with active gastritis who were on PPI (Protein Pump Inhibitor) as gas-reducing drugs were included in our study.
Participants were verbally informed about the study, and written consent was obtained from eligible patients. Then, the questions were asked as per our questionnaire format to obtain the data on age, sex, education, address, source of drinking water, and others. Blood samples were collected in plain tubes labeled with unique code numbers and centrifuged to get serum. The samples were processed at the Microbiology Laboratory of the School of Health and Allied Sciences, Pokhara University. The samples were processed for antibodies against H. pylori by a rapid diagnostic kit based on immunochromatographic methods, which were manufactured by CTK Diagnostics, China. Two to three drops of serum sample were placed in the sample wells by the dropper given in the kit, and the diluter was placed in D wells. The samples started to move, and the reading commenced within five minutes. If there was line formation in the test and control, it was regarded as positive; if there was a line formation in only the control line, the test was negative; if the line was formed at the test only, then the test was invalid.
Ethical permission was obtained from the Institutional Review Committee, Pokhara University, for ethical clearance (Ref no. 197/074/75). The permission was obtained from the Pokhara Metropolitan-30 ward office.
All of the data was analyzed using SPSS version 16.0. The frequency of incidence of different independent variables and dependent variables was calculated. Correlation between measured parameters was assessed using the analytical methods of Pearson’s Chi-square test, and p<0.05 was considered statistically significant.
Results
The present study was conducted on 150 participants with active gastritis. Active gastritis was confined by those who were taking anti-gastritis drugs to reduce the gas formation on a daily basis in the Lekhnath community, now known as Pokhara-30. H. Pylori antibodies were used for H. pylori infection diagnosis for all participants, along with their history and socio-demographic information. All participants were provided with the reports, and positive cases were advised for follow-up. In this study, out of 150 participants, 3 (2.0%) were of age group <20 years, 17 (11.3%) were 20 to 30 years, 51(34.0%) were 30 to 40 years, and 79 (52.7%) were >40 years. Similarly, 96 (64%) females and 54 (36%) males were included in our study. This study included 142 (94.7%) married and 8 (5.3%) unmarried individuals, and other details are demonstrated in Table 1. Similarly, H. pylori antibody was detected to identify the status of infectious gastritis of participants during the study. In this regard, 103 (68.7%) were negative for H. pylori, and 47 (31.3%) were positive, which demonstrated the infection as the cause of gastritis.
Associations were seen in different variables, as given in the tables below. Out of 47 positive cases of H. pylori, in terms of age, the prevalence was highest in the 30 to 40-year-old age group (14.0%). The prevalence was higher in females with 32 (21.3%) than in males with 15 (10.0%). Similarly, the prevalence was highest in people living in Khudi (18.0%) among four test areas of Lekhnath-30. Participants who were married showed the highest prevalence of 44 (29.3%) compared to unmarried participants 3(2.0%). There was a significant relationship between H. pylori infection and occupation, with a P-value of 0.05, and the prevalence was highest among housewives. Similarly, the condition was more prevalent among 15 individuals who had a middle school education (10.0%), as demonstrated in Table 1.
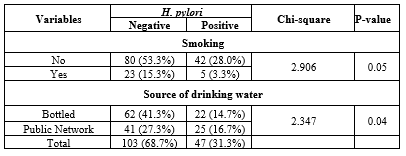
H. pylori infection was strongly associated with the consumption of various qualities of water. Among 47 (31.3%) individuals with H. pylori, 22(14.7%) consumed bottled water, whereas 25(16.7%) used running water, which showed a strong association with P-value 0.04, as shown in Table 2. Anti-gas-reducing drugs showed a statistically significant association with H. pylori, as shown in Table 3.
Discussion
This is a cross-sectional study on individuals with active gastritis. In our study, a total number of 150 samples was collected. Out of 150 samples, 47 (31.3%) were found to be positive and 103 (68.7%) negatives for H. pylori. The age group 30 to 40 years showed the highest prevalence of (14.0%) comparatively more than 40 years age group (12.7%) and 20-30 years age group (4.7%). The prevalence was higher in females, 32 individuals (21.3%), than in males, 15 participants (10.0%).
The prevalence of H. pylori among individuals with active gastritis was lower in our study (31.3%) than in the study by Agbor et al., which reported 43.4% (19). Moreover, H. pylori infections are comparatively more prevalent in studies conducted by Zhu et al. 63.41% (20), Mynepalli et al. 59.0% (21), and Adlekha et al. 59.4% (22). However, Awuku et al. (23) found a lower prevalence of 14.2% than our study. Similarly, a previous study by Hoang et al. in Vietnam reported a seroprevalence of 36.7% (24) and Correa et al. 36.4% (25), which are comparatively similar to our study. These differences in prevalence may be due to the improvement in the socioeconomic status and hygiene condition of the society over time.
In terms of age, the prevalence was higher in the age group 30 to 40 years (14.0%) than older than 40 years age group (12.7%) and the group between 20 and 30 (4.7%) and was lowest in the age group younger than 20 (0.0%). This may be due to the aging process, which is associated with a diminished epithelial cell turnover rate and reduced capacity to repair the gastric mucosa (26), which has been attributed to decreasing prostaglandin levels in the gastric mucosa, which makes age a major risk factor for H. pylori colonization (27). WHO has reported that the majority of infections occurred in young and middle age groups (25 to 50 years) more than in other age groups, and the factors that predispose the higher colonization rates included poor socioeconomic status and less education in addition to genetic factors. The prevalence was higher in females (68 %) than in males (32 %), which is similar to a study by Mynepalli et al. et al. 62.7% (21) and Agbor et al. 45.5 % (19). Participants who were married, 44 persons, showed a higher prevalence (29.3%) than the unmarried ones, who were 3 (2.0%).
Similarly, there was no association between alcohol consumption and H. pylori infection in our study. However, a study by Agbor et al. showed that H. pylori infection was higher among alcohol consumers (51.1%) than among those who had never drunk (40.3%) (19). Similarly, the infection rate was higher among smokers than non-smokers, which is similar to the study done by Hanafi MI et al. (28). This suggests that smoking may also be a risk factor for H. pylori infection. Higher prevalence was found among individuals who consumed public running water instead of pure bottled water.
Conclusion
Although the participants used gastric drugs, the prevalence of H. pylori in these individuals was higher. H. pylori was more prevalent among females than males and was more common in the age group 30 to 40 years. The result of our research highlights the importance of periodic screening and checkups in order to detect the infecting agent among active gastritis patients. Complete cure of infective gastritis requires anti-H. pylori drugs and gastritis drugs are insufficient on their own.
Public awareness and health education programs are necessary to heighten the awareness of people with gastritis and its consequences, including ulcers. Awareness-raising campaigns should be focused on sanitation and prevention control of H. pylori infection.
Limitation
Since this study was focused on a small population large scale population should be focused to carry the research. Other tests like molecular testing were not carried.
Acknowledgement
The authors would like to express their gratitude to the Pokhara University Research Centre and ward office for granting permission to conduct the study. The authors would like to express their gratitude to all the participants who directly and indirectly contributed to the success of this research.
Funding sources
The Pokhara University Research Centre funded this research project through the Faculty Research Grant.
Ethical statement
Ethical permission was obtained from the Pokhara University Research Centre (Ref no. 197/074/75) to undertake the study.
Conflicts of interest
The authors declare no conflict of interest.
Author contributions
Suresh Jaiswal and Bijay Subedi: Conceptualization, Methodology, Data Analysis, Writing, and Editing: Ashmita Sapkota, Pushpa Sharma, Manisha Timisina and Maheshwar Timilsina: Investigation, Data collection, Data analysis, and Writing (Original Draft). Bishnu raj Tiwari: Editing original draft.
Helicobacter pylori (H. pylori) is a spiral-shaped microaerophilic gram-negative bacterium (1). It is helix-shaped, which is thought to have evolved to penetrate the mucous lining of the stomach (2). It leads to the development of chronic gastritis, gastric ulcers, duodenal ulcers, and mucosal atrophy. Additionally, Helicobacter pylori is recognized as a class I cancer-causing agent because long-lasting inflammation and atrophy can further lead to malignant transformation (3, 4). At least half the world’s population is infected by this bacterium, making it the most widespread infection in the world, especially in the developing world, where rates are estimated to be around 80% (5).
H. pylori infection is an important global infection with a worldwide prevalence of about 50 % (6, 7). This infection is mostly acquired during childhood through the fecal-oral and oral-oral routes (8, 9). Early infection with this bacterium is usually silent, but symptoms and pathologic changes occur later in life. The clinical conditions and pathologic changes associated with H. pylori infection include gastritis, gastric and duodenal ulcers, gastric cancers, iron deficiency anemia, and idiopathic thrombocytopenic purpura (ITP) (10-13).
H. pylori infection shows a variety of geographic distribution on both local communities and large global scales. These variations are mostly due to socioeconomically driven factors such as sex, age, genetic tendency, ethnicity, level of education, and sanitation, which decide the rate and prevalence of this worldwide infection (14-16).
In developing countries, H. pylori is found to be the most common human infection globally. In developing countries, more than 80% of the population test positive for H. pylori (14,17,18).
The main objective of this study was to determine the H. pylori infection in the population of Lekhnath municipality of Kaski district to assess the risk factors for H. pylori by an extended anamnesis, involving data on sex, age, educational level, smoking, drinking, as well as dietary factors.
Methods
A community-based cross-sectional study was carried out from 2018/5/7 to 2019/03/01 at Pokhara 30, earlier known as Lekhnath. Samples were collected from Khudi, Dhungepatan, and the Powerhouse area of Pokhara-30. Only those with active gastritis who were on PPI (Protein Pump Inhibitor) as gas-reducing drugs were included in our study.
Participants were verbally informed about the study, and written consent was obtained from eligible patients. Then, the questions were asked as per our questionnaire format to obtain the data on age, sex, education, address, source of drinking water, and others. Blood samples were collected in plain tubes labeled with unique code numbers and centrifuged to get serum. The samples were processed at the Microbiology Laboratory of the School of Health and Allied Sciences, Pokhara University. The samples were processed for antibodies against H. pylori by a rapid diagnostic kit based on immunochromatographic methods, which were manufactured by CTK Diagnostics, China. Two to three drops of serum sample were placed in the sample wells by the dropper given in the kit, and the diluter was placed in D wells. The samples started to move, and the reading commenced within five minutes. If there was line formation in the test and control, it was regarded as positive; if there was a line formation in only the control line, the test was negative; if the line was formed at the test only, then the test was invalid.
Ethical permission was obtained from the Institutional Review Committee, Pokhara University, for ethical clearance (Ref no. 197/074/75). The permission was obtained from the Pokhara Metropolitan-30 ward office.
All of the data was analyzed using SPSS version 16.0. The frequency of incidence of different independent variables and dependent variables was calculated. Correlation between measured parameters was assessed using the analytical methods of Pearson’s Chi-square test, and p<0.05 was considered statistically significant.
Results
The present study was conducted on 150 participants with active gastritis. Active gastritis was confined by those who were taking anti-gastritis drugs to reduce the gas formation on a daily basis in the Lekhnath community, now known as Pokhara-30. H. Pylori antibodies were used for H. pylori infection diagnosis for all participants, along with their history and socio-demographic information. All participants were provided with the reports, and positive cases were advised for follow-up. In this study, out of 150 participants, 3 (2.0%) were of age group <20 years, 17 (11.3%) were 20 to 30 years, 51(34.0%) were 30 to 40 years, and 79 (52.7%) were >40 years. Similarly, 96 (64%) females and 54 (36%) males were included in our study. This study included 142 (94.7%) married and 8 (5.3%) unmarried individuals, and other details are demonstrated in Table 1. Similarly, H. pylori antibody was detected to identify the status of infectious gastritis of participants during the study. In this regard, 103 (68.7%) were negative for H. pylori, and 47 (31.3%) were positive, which demonstrated the infection as the cause of gastritis.
Associations were seen in different variables, as given in the tables below. Out of 47 positive cases of H. pylori, in terms of age, the prevalence was highest in the 30 to 40-year-old age group (14.0%). The prevalence was higher in females with 32 (21.3%) than in males with 15 (10.0%). Similarly, the prevalence was highest in people living in Khudi (18.0%) among four test areas of Lekhnath-30. Participants who were married showed the highest prevalence of 44 (29.3%) compared to unmarried participants 3(2.0%). There was a significant relationship between H. pylori infection and occupation, with a P-value of 0.05, and the prevalence was highest among housewives. Similarly, the condition was more prevalent among 15 individuals who had a middle school education (10.0%), as demonstrated in Table 1.
|
Table 1. The relationship between age and sex of the participants and H. pylori
 |
|
Table 2. The association between H. pylori, smoking habits, and the source of drinking water
 |
|
Table 3. Association of H pylori with gas-reducing drugs
 |
Discussion
This is a cross-sectional study on individuals with active gastritis. In our study, a total number of 150 samples was collected. Out of 150 samples, 47 (31.3%) were found to be positive and 103 (68.7%) negatives for H. pylori. The age group 30 to 40 years showed the highest prevalence of (14.0%) comparatively more than 40 years age group (12.7%) and 20-30 years age group (4.7%). The prevalence was higher in females, 32 individuals (21.3%), than in males, 15 participants (10.0%).
The prevalence of H. pylori among individuals with active gastritis was lower in our study (31.3%) than in the study by Agbor et al., which reported 43.4% (19). Moreover, H. pylori infections are comparatively more prevalent in studies conducted by Zhu et al. 63.41% (20), Mynepalli et al. 59.0% (21), and Adlekha et al. 59.4% (22). However, Awuku et al. (23) found a lower prevalence of 14.2% than our study. Similarly, a previous study by Hoang et al. in Vietnam reported a seroprevalence of 36.7% (24) and Correa et al. 36.4% (25), which are comparatively similar to our study. These differences in prevalence may be due to the improvement in the socioeconomic status and hygiene condition of the society over time.
In terms of age, the prevalence was higher in the age group 30 to 40 years (14.0%) than older than 40 years age group (12.7%) and the group between 20 and 30 (4.7%) and was lowest in the age group younger than 20 (0.0%). This may be due to the aging process, which is associated with a diminished epithelial cell turnover rate and reduced capacity to repair the gastric mucosa (26), which has been attributed to decreasing prostaglandin levels in the gastric mucosa, which makes age a major risk factor for H. pylori colonization (27). WHO has reported that the majority of infections occurred in young and middle age groups (25 to 50 years) more than in other age groups, and the factors that predispose the higher colonization rates included poor socioeconomic status and less education in addition to genetic factors. The prevalence was higher in females (68 %) than in males (32 %), which is similar to a study by Mynepalli et al. et al. 62.7% (21) and Agbor et al. 45.5 % (19). Participants who were married, 44 persons, showed a higher prevalence (29.3%) than the unmarried ones, who were 3 (2.0%).
Similarly, there was no association between alcohol consumption and H. pylori infection in our study. However, a study by Agbor et al. showed that H. pylori infection was higher among alcohol consumers (51.1%) than among those who had never drunk (40.3%) (19). Similarly, the infection rate was higher among smokers than non-smokers, which is similar to the study done by Hanafi MI et al. (28). This suggests that smoking may also be a risk factor for H. pylori infection. Higher prevalence was found among individuals who consumed public running water instead of pure bottled water.
Conclusion
Although the participants used gastric drugs, the prevalence of H. pylori in these individuals was higher. H. pylori was more prevalent among females than males and was more common in the age group 30 to 40 years. The result of our research highlights the importance of periodic screening and checkups in order to detect the infecting agent among active gastritis patients. Complete cure of infective gastritis requires anti-H. pylori drugs and gastritis drugs are insufficient on their own.
Public awareness and health education programs are necessary to heighten the awareness of people with gastritis and its consequences, including ulcers. Awareness-raising campaigns should be focused on sanitation and prevention control of H. pylori infection.
Limitation
Since this study was focused on a small population large scale population should be focused to carry the research. Other tests like molecular testing were not carried.
Acknowledgement
The authors would like to express their gratitude to the Pokhara University Research Centre and ward office for granting permission to conduct the study. The authors would like to express their gratitude to all the participants who directly and indirectly contributed to the success of this research.
Funding sources
The Pokhara University Research Centre funded this research project through the Faculty Research Grant.
Ethical statement
Ethical permission was obtained from the Pokhara University Research Centre (Ref no. 197/074/75) to undertake the study.
Conflicts of interest
The authors declare no conflict of interest.
Author contributions
Suresh Jaiswal and Bijay Subedi: Conceptualization, Methodology, Data Analysis, Writing, and Editing: Ashmita Sapkota, Pushpa Sharma, Manisha Timisina and Maheshwar Timilsina: Investigation, Data collection, Data analysis, and Writing (Original Draft). Bishnu raj Tiwari: Editing original draft.
Research Article: Research Article |
Subject:
Microbiology
Received: 2023/05/14 | Accepted: 2023/09/12 | Published: 2024/01/25 | ePublished: 2024/01/25
Received: 2023/05/14 | Accepted: 2023/09/12 | Published: 2024/01/25 | ePublished: 2024/01/25
References
1. Wang YC, Lin TY, Shang ST, Chen HJ, Kao CH, Wu CC, et al. Helicobacter pylori infection increases the risk of adult-onset asthma: a nationwide cohort study. Eur J Clin Microbiol Infect Dis. 2017;36(9):1587-94. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Diaconu S, Predescu A, Moldoveanu A, Pop CS, Fierbințeanu-Braticevici C. Helicobacter pylori infection: old and new. J Med Life. 2017;10(2):112-7. [View at Publisher] [PMID] [Google Scholar]
3. Gomceli I, Demiriz B, Tez M. Gastric carcinogenesis. World J Gastroenterol. 2012;18(37):5164. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Fox JG, Wang TC. Inflammation, atrophy, and gastric cancer. Journal of Clinical Investigation. 2007;117(1):60-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Porras C, Nodora J, Sexton R, Ferreccio C, Jimenez S, Dominguez RL, et al. Epidemiology of Helicobacter pylori infection in six Latin American countries (SWOG Trial S0701). Cancer Causes Control. 2013;24:209-15. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Gravina AG, Zagari RM, De Musis C, Romano L, Loguercio C, Romano M. Helicobacter pylori and extragastric diseases: A review. World J Gastroenterol. 2018;24(29):3204-21. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Guevara B, Cogdill AG. Helicobacter pylori: a review of current diagnostic and management strategies. Digestive Diseases and Sciences. 2020;65:1917-31. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Malaty HM, El-Kasabany A, Graham DY, Miller CC, Reddy SG, Srinivasan SR, et al. Age at acquisition of Helicobacter pylori infection: a follow-up study from infancy to adulthood. Lancet. 2002;359(9310):931-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Dunne C, Dolan B, Clyne M. Factors that mediate colonization of the human stomach by Helicobacter pylori. World J Gastroenterol. 2014;20(19):5610-24. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Galal YS, Ghobrial CM, Labib JR, Abou-Zekri ME. Helicobacter pylori among symptomatic Egyptian children: prevalence, risk factors, and effect on growth. J Egypt Public Health Assoc. 2019;94:1-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Stefano K, Marco M, Federica G, Laura B, Barbara B, Gioacchino L, et al. Helicobacter pylori, transmission routes and recurrence of infection: state of the art. Acta Biomed. 2018;89(Suppl 8):72-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Kuwana M. Helicobacter pylori-associated immune thrombocytopenia: clinical features and pathogenic mechanisms. World J Gastroenterol. 2014;20(3):714-23. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Franchini M, Cruciani M, Mengoli C, Pizzolo G, Veneri D. Effect of Helicobacter pylori eradication on platelet count in idiopathic thrombocytopenic purpura: a systematic review and metaanalysis. J Antimicrob Chemother. 2017;60(2):237-46. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Zabala Torrres B, Lucero Y, Lagomarcino AJ, Orellana‐Manzano A, George S, Torres JP, et al. Prevalence and dynamics of Helicobacter pylori infection during childhood. Helicobacter. 2017;22(5):e12399. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Leja M, Grinberga‐Derica I, Bilgilier C, Steininger C. Epidemiology of Helicobacter pylori infection. Helicobacter. 2019;24(1):e12635. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Archampong TN, Asmah RH, Wiredu E, Gyasi RK, Nkrumah KN, Rajakumar K. Epidemiology of Helicobacter pylori infection in dyspeptic Ghanaian patients. Pan Afr Med J. 2015;20:178. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Kim SE, Park MI, Park SJ, Moon W, Choi YJ, Cheon JH, et al. Trends in Helicobacter pylori eradication rates by first-line triple therapy and related factors in eradication therapy. Korean J Intern Med. 2015;30(6):801-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Jemilohun AC, Otegbayo JA, Ola SO, Oluwasola AO, Akere A. Diagnostic accuracy of rapid urease test for the diagnosis of Helicobactor pylori in gastric biopsies in Nigerians with dyspepsia. African J Clin Exper Microbiol. 2011;12(2):62-6. [View at Publisher] [DOI] [Google Scholar]
19. Zabala Torrres B, Lucero Y, Lagomarcino AJ, Orellana‐Manzano A, George S, Torres JP, et al. Prevalence and dynamics of Helicobacter pylori infection during childhood. Helicobacter. 2017;22(5):e12399. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Agbor NE, Esemu SN, Ndip LM, Tanih NF, Smith SI, Ndip RN. Helicobacter pylori in patients with gastritis in West Cameroon: prevalence and risk factors for infection. BMC research notes. 2018;11(1):559. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Zhu Y, Zhou X, Wu J, Su J, Zhang G. Risk factors and prevalence of Helicobacter pylori infection in persistent high incidence area of gastric carcinoma in Yangzhong city. Gastroenterology Research and Practice. 2014;2014. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Correa S, Cardona AF, Correa T, Correa LA, García HI, Estrada S. Prevalence of Helicobacter pylori and Histopathological Features in Gastric Biopsies from Patients with Dyspeptic Symptoms at a Referral Center in Medellin. RevistaColombiana de Gastroenterologia. 2016;31(1):9-15. [View at Publisher] [DOI] [Google Scholar]
23. Mynepalli SK, Maureen O, Mumuni A. Prevalence of Helicobacter pylori and hygiene practices among public secondary school students in Ikeja Local Government Area, Lagos, Nigeria. Health. 2014;6(04):250. [View at Publisher] [DOI] [Google Scholar]
24. Adlekha S, Chadha T, Krishnan P, Sumangala B. Prevalence of helicobacter pylori infection among patients undergoing upper gastrointestinal endoscopy in a medical college hospital in kerala, India. Annals of medical and health sciences research. 2013;3(4):559-63. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Awuku YA, Simpong DL, Alhassan IK, Tuoyire DA, Afaa T, Adu P. Prevalence of helicobacter pylori infection among children living in a rural setting in Sub-Saharan Africa. BMC public health. 2017;17(1):1-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Pucułek M, Machlowska J, Wierzbicki R, Baj J, Maciejewski R, Sitarz R. Helicobacter pylori associated factors in the development of gastric cancer with special reference to the early-onset subtype. Oncotarget. 2018;9(57):31146-62. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Pilotto A, Franceschi M. Helicobacter pylori infection in older people. World J Gastroenterol. 2014;20(21):6364-73. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Sostres C, Gargallo CJ, Lanas A. Interaction between Helicobacter pylori infection, nonsteroidal anti-inflammatory drugs and/or lowdose aspirin use: old question new insights. World J Gastroenterol. 2014;20(28):9439-50. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Hanafi MI, Mohamed AM. Helicobacter pylori infection: seroprevalence and predictors among healthy individuals in Al Madinah, Saudi Arabia. J Egypt Public Health Assoc. 2013;88(1):40-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.