
Thu, May 29, 2025
Volume 18, Issue 6 (Nov-Dec 2024)
mljgoums 2024, 18(6): 1-4 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Atulbhai Contractor T, Parsotambhai Thakkar H, Ishwar Dayal A, Omprakash Agrawal S, Kamleshbhai Patel H. Histopathological spectrum of upper-gastrointestinal lesions on endoscopic biopsies. mljgoums 2024; 18 (6) :1-4
URL: http://mlj.goums.ac.ir/article-1-1820-en.html
URL: http://mlj.goums.ac.ir/article-1-1820-en.html
Tejas Atulbhai Contractor1 

 , Himali Parsotambhai Thakkar2 , Anupama Ishwar Dayal3 , Sandesh Omprakash Agrawal1 , Hani Kamleshbhai Patel1
, Himali Parsotambhai Thakkar2 , Anupama Ishwar Dayal3 , Sandesh Omprakash Agrawal1 , Hani Kamleshbhai Patel1
, Himali Parsotambhai Thakkar2 , Anupama Ishwar Dayal3 , Sandesh Omprakash Agrawal1 , Hani Kamleshbhai Patel1
1- Department of Pathology, GCS Medical College Hospital and Research Center, Ahmedabad, Gujarat, India
2- Shraddha Pathology Laboratory, Ahmedabad, Gujarat, India
3- Department of Pathology, GCS Medical College Hospital and Research Center, Ahmedabad, Gujarat, India ,anupamadayal2019@gmail.com
2- Shraddha Pathology Laboratory, Ahmedabad, Gujarat, India
3- Department of Pathology, GCS Medical College Hospital and Research Center, Ahmedabad, Gujarat, India ,
Full-Text [PDF 479 kb]
(361 Downloads)
| Abstract (HTML) (1006 Views)
Discussion
Upper GI lesions are major causes of morbidity. Endoscopy visualizes and biopsies mucosal lesions, being minimally invasive and outpatient (4).
In the present study, the majority of the samples are from the esophagus, comprising 48.5%, followed by an equal number of cases from the stomach and duodenum, each comprising 25.7%. A study by Sharma et al. also showed that the majority of samples were from the esophagus, whereas other studies by Qureshi et al. (5), Vidyavathi et al. (6), Kothari et al. (7), Krishnappa et al. (8), Hussain et al. (2), and Abilash et al. (9) show that the majority of biopsies were from the stomach.
Demographic data related to age and sex in the present study show trends almost similar to those in other reported studies: Qureshi et al. (5), UK; Sacco et al. (10), USA; Vidyavathi et al. (6), India (Kolar); Krishnappa et al. (8), Bangalore; Hussain et al. (2), Kerala; and Abilash et al. (9), Srinagar, all showing male predominance. However, Choomsri et al. (11) reported female preponderance. The present study shows the highest number of upper GI endoscopic biopsies in the 5th and 6th decades of life, similar to other studies that also show a preponderance between 40-60 years of age. The reason for this finding is that males are comparatively more exposed to environmental pollutants than females and are more involved in habits such as smoking and tobacco consumption than females (12).
The present study shows a mild predominance of non-neoplastic lesions of the upper GI tract (52.4%), which is similar to other studies like Qureshi et al. (5) (17%), Krishnappa et al. (8) (44%), and Abilash et al. (9) (22%). However, other studies, such as those by Vidyavathi (6) and Hussain (2), show a predominance of neoplastic lesions.
Chronic nonspecific oesophagitis (10.5%) was the most common diagnosis, similar to the studies by Qureshi et al. (5), Krishnappa et al. (8), and Abilash et al. (9). Abhilash et al. (9) and Kothari et al. (7) reported 1% and 1.5% of cases of Barrett’s esophagus, respectively. Ulceration is nearly always induced by gastroesophageal reflux and is reported to occur in 10% of patients with this condition. The main complications of Barrett’s esophagus include peptic ulcer, stricture, bleeding, and the development of dysplasia and adenocarcinoma (Table 4).
Dysplasia is found in Barrett’s esophagus in the absence of carcinoma in 5-10% of the cases and is associated with carcinoma in 68-100% of the cases. Malignant lesions were more common, accounting for 74.5% of the total esophageal biopsies (n=51), while 25.5% were non-neoplastic lesions. Similar findings were observed in studies conducted by Qureshi et al. (5) and Hussain et al. (2).
The American College of Gastroenterology recommends 1-year endoscopy for Barrett's mucosa, 6 months for low-grade dysplasia, and then yearly follow-ups. High-grade dysplasia patients require expert confirmation, repeat endoscopy within three months, and biopsies to exclude carcinoma from flat mucosa (2). Esophageal squamous dysplasia predicts esophageal squamous cell carcinoma. Found in ≥25% of adults above 35 years, it parallels carcinoma rates (13). Squamous cell carcinoma (71%) was the most common histological type in the malignant lesions, which is comparable to various studies (9,14,15) reporting rates ranging from 66% to 100%. In addition, 52.6% of patients with esophageal carcinoma were in the 56-75-year age group. These observations align with studies by Abhilash et al. (9) and Qureshi et al. (5). Esophageal cancer ranks eighth in incidence and sixth in mortality globally (16). Dawsey et al. (17) note that, in the West, adenocarcinoma is rising, while squamous cell carcinoma remains predominant elsewhere. Parkin et al. (16) state that 80% of esophageal carcinomas occur in developing countries, mostly esophageal squamous cell carcinoma. In India, it ranks as the third and fourth leading cancer in men and women, respectively (18).
In this study, overall inflammatory lesions were more prevalent in stomach biopsies, with chronic nonspecific gastritis being the most common diagnosis.
Memon et al. (19) and Gumber et al. (15) also showed similar trends. Gastritis with intestinal metaplasia or dysplasia is a significant histological finding, indicating a premalignant disease. In 11.1% of the cases, intestinal metaplasia/dysplasia was seen along with gastritis. A similar observation was also made by Abhilash et al. (9) and Krishnappa et al. (8). Only 8.5% of the gastric biopsies were diagnosed as malignancy on histology, adenocarcinoma being the histological type. Memon et al. (19) and Abhilash et al. (9) also reported a lower prevalence of malignancy, with frequencies of 5% and 7.5%, respectively.
Non-specific duodenitis was the most common lesion encountered in the duodenum. The duodenum has a rich, rapidly regenerating epithelial lining that can easily be affected by any inflammatory insult (19). The prevalence of inflammatory lesions in the duodenum was also demonstrated in studies by Abhilash et al. (9), Qureshi et al. (5), Hussain et al. (2), Krishnappa et al. (8), and Kothari et al. (7).
In this study, 33.3% of the cases had celiac disease. The Marsh-Oberhuber criteria, based on small bowel biopsies, are used for grading (20). Increased intraepithelial T lymphocytes suggest celiac disease even in the absence of villous atrophy (3). In this study, Type III (66.6%) was the most common, while Type I (11.1%) was the least common. In contrast, Memon (19) reported 76.1% of cases with suspected celiac disease, with mild cases being more prevalent. Difficulty in identifying intraepithelial T lymphocytes due to small biopsies may explain the lower number of Type I cases. Malignant cases in the duodenum were rare (1.9%), consistent with findings from other studies by Krishnappa et al. (8), Raychaudhuri et al. (21), and Khandige et al. (22).
Conclusion
This study highlights endoscopic patterns correlated with histopathology for early detection and treatment. It provides valuable insights into the demographic distribution, lesion types, and comparisons with other studies, aiding in understanding regional trends and advancing diagnostic approaches. Histopathology is crucial in assessing upper GI lesions from endoscopic biopsies, distinguishing between non-neoplastic, premalignant, and neoplastic conditions, especially in Barrett's esophagus. Esophageal biopsies were common, with malignancy in 47.6%, predominantly in the esophagus, particularly in those aged 50-60. Gastric and duodenal lesions are often benign, but suspicion and timely histopathological study aid early management. Accurate diagnosis improves patient outcomes while understanding lesion demographics aids in tailoring management. The synergy between endoscopy and histopathology enhances diagnostic precision, guiding optimal clinical decisions and improving care.
Acknowledgement
The authors extend their sincere appreciation to the management and all staff in the Department of Pathology, Medical College and Research Center, Ahmedabad, Gujarat, where this study was conducted.
Funding sources
No funding sources.
Ethical statement
The study was approved by the Institutional Ethics Committee (GCSMC/EC/Dissertation/APPROVE/2019/0091).
Conflicts of interest
None declared.
Author contributions
All the authors have participated in one or more parts of the present study: Anupama Ishwar Dayal conducted the test; Tejas Atulbhai Contractor and Himali Parsotambhai Thakkar performed the data analysis and wrote the manuscript; Sandesh Omprakash Agrawal and Hani Kamleshbhai Patel collected the data.
Full-Text: (132 Views)
Introduction
Upper gastrointestinal (GI) lesions significantly contribute to global morbidity, ranging from benign inflammatory conditions to malignant neoplasms (1). This study examines the demographic distribution of upper GI lesions by age, sex, and biopsy site, focusing on the esophagus, stomach, and duodenum. It compares the prevalence of neoplastic and non-neoplastic lesions, emphasizing the importance of premalignant conditions like Barrett's esophagus (Where columnar cells replace squamous mucosa after ulceration, arising from gastric migration or stem cell changes) and malignancies such as esophageal squamous cell carcinoma and gastric adenocarcinoma (2). Common inflammatory conditions, including esophagitis (Eosinophilic esophagitis involves ≥15 eosinophils per field, while infectious esophagitis arises from various pathogens), gastritis (Acute gastritis involves inflammation; chronic gastritis includes autoimmune or H. pylori-associated glandular atrophy and metaplasia), and duodenitis (Duodenitis is graded by neutrophil and plasma cell infiltration, villous height, and gastric metaplasia), are also analyzed alongside rarer findings like celiac disease and neuroendocrine tumors (3). Early detection, especially of premalignant and malignant lesions, is essential for timely intervention and management. Endoscopy plays a pivotal role as a minimally invasive method for visualizing and biopsy lesions in the upper GI tract.
Methods
This descriptive cross-sectional study conducted at a tertiary care center in Gujarat, India, from July 2019 to October 2021, analyzed 104 upper GI endoscopic biopsies from patients with upper GI symptoms, excluding lesions of the mouth and pharynx, distal duodenal biopsies, and inadequately preserved specimens. Most esophageal and gastric biopsies were from thickened, friable, or ulcerated areas in the middle and lower esophagus. Duodenal biopsies were from the second part (D2), showing scalloping or nodularity. Tissues were processed, stained, and analyzed microscopically. Special stains were used to confirm H. pylori and other lesions. Malignant lesions were classified according to the WHO guidelines, and duodenal biopsies for suspected celiac disease were graded using the Modified Marsh Oberhuber classification.
Results
Age and site-wise distribution of upper GI lesions shows that the maximum biopsies were obtained from the age group of 46-55 years, followed by the 66-75 age group, with a male to female ratio of 1.7:1 (Figure 1). Out of a total of 104 endoscopic biopsy specimens, the majority (50/104) were from the esophagus, followed by 27 each from the stomach and duodenum, with one biopsy from the gastroesophageal junction.
Upper gastrointestinal (GI) lesions significantly contribute to global morbidity, ranging from benign inflammatory conditions to malignant neoplasms (1). This study examines the demographic distribution of upper GI lesions by age, sex, and biopsy site, focusing on the esophagus, stomach, and duodenum. It compares the prevalence of neoplastic and non-neoplastic lesions, emphasizing the importance of premalignant conditions like Barrett's esophagus (Where columnar cells replace squamous mucosa after ulceration, arising from gastric migration or stem cell changes) and malignancies such as esophageal squamous cell carcinoma and gastric adenocarcinoma (2). Common inflammatory conditions, including esophagitis (Eosinophilic esophagitis involves ≥15 eosinophils per field, while infectious esophagitis arises from various pathogens), gastritis (Acute gastritis involves inflammation; chronic gastritis includes autoimmune or H. pylori-associated glandular atrophy and metaplasia), and duodenitis (Duodenitis is graded by neutrophil and plasma cell infiltration, villous height, and gastric metaplasia), are also analyzed alongside rarer findings like celiac disease and neuroendocrine tumors (3). Early detection, especially of premalignant and malignant lesions, is essential for timely intervention and management. Endoscopy plays a pivotal role as a minimally invasive method for visualizing and biopsy lesions in the upper GI tract.
Methods
This descriptive cross-sectional study conducted at a tertiary care center in Gujarat, India, from July 2019 to October 2021, analyzed 104 upper GI endoscopic biopsies from patients with upper GI symptoms, excluding lesions of the mouth and pharynx, distal duodenal biopsies, and inadequately preserved specimens. Most esophageal and gastric biopsies were from thickened, friable, or ulcerated areas in the middle and lower esophagus. Duodenal biopsies were from the second part (D2), showing scalloping or nodularity. Tissues were processed, stained, and analyzed microscopically. Special stains were used to confirm H. pylori and other lesions. Malignant lesions were classified according to the WHO guidelines, and duodenal biopsies for suspected celiac disease were graded using the Modified Marsh Oberhuber classification.
Results
Age and site-wise distribution of upper GI lesions shows that the maximum biopsies were obtained from the age group of 46-55 years, followed by the 66-75 age group, with a male to female ratio of 1.7:1 (Figure 1). Out of a total of 104 endoscopic biopsy specimens, the majority (50/104) were from the esophagus, followed by 27 each from the stomach and duodenum, with one biopsy from the gastroesophageal junction.
.PNG)
Based on the findings, the endoscopic biopsies were categorized into non-neoplastic and neoplastic lesions, with 55 cases (52.8%) and 49 cases (47.1%), respectively. Among the non-neoplastic lesions, the maximum number of cases (25 cases, 24%) were from the duodenum. Among the neoplastic lesions, the highest number of cases were from the esophagus (38 cases, 36.5%). Findings of endoscopy and histopathology of non-neoplastic and neoplastic lesions of the esophagus and gastroesophageal junction are provided in Table 1.
The results show that the maximum biopsies from the esophagus were obtained from the age group of 56-65 years, with a male to female ratio of 1.2:1. Out of the total 50 cases (n=12), 24% were non-neoplastic and 76% (n=38) were neoplastic. There were an equal number of benign lesions in both sexes, while malignant lesions were more common in males compared to females, with a male to female ratio of 1.3:1. Out of the 12 (24%) non-neoplastic cases, 11 (21.6%) were cases of esophagitis, and one case was Barrett’s esophagus. A total of 38 (74.5%) cases were neoplastic. Among the neoplastic cases, all were malignant, with squamous cell carcinoma being the most common (Figure 2). Of the 11 cases of esophagitis, the maximum cases presented with erythematous changes on endoscopy. One case of Barrett’s esophagus presented as an ulcerative lesion. Ulceration with proliferative growth was commonly seen in squamous cell carcinomas, whereas ulceration was not commonly associated with adenocarcinoma. Adenocarcinoma presented as a proliferative lesion with or without ulceration.
The maximum biopsies from the stomach were obtained from the age group of 66-75 years, with a male to female ratio of 1.7:1. Out of the total 27 cases (n=18), benign lesions were more common, accounting for 66.7%, while 33.3% were malignant. Both benign and malignant lesions were more common in male patients. The most common benign lesion was gastritis (Figure 2), accounting for 48.1%, which peaked in the 66-75 years age group. Adenocarcinoma (Figure 2) was the most common malignant lesion, peaking in the 46-55 years age group.
Out of 13 cases of gastritis, nine cases presented as erythematous changes on endoscopy. The maximum cases (Six cases) of adenocarcinoma presented as an ulcer-proliferative growth on endoscopy, while hyperplastic polyps presented as polypoidal growths on endoscopy (Table 2).
The maximum biopsies of the duodenum were received from the 46-55 years age group, with a male to female ratio of 3.5:1. Out of 27 biopsies, the majority of the lesions were benign (25 cases, 92.6%), and two cases (7.4%) were neoplastic. Duodenitis (48%, 13/25) was the most common benign lesion encountered, followed by 33.3% of cases of celiac disease (Figure 2), hyperplastic polyp (7.4%), and a single case of tropical sprue. There were two cases of malignant duodenal lesions seen in elderly male patients (56-75 years). One patient had adenocarcinoma (Figure 2), and one had a well-differentiated neuroendocrine neoplasm.
The results show that the maximum biopsies from the esophagus were obtained from the age group of 56-65 years, with a male to female ratio of 1.2:1. Out of the total 50 cases (n=12), 24% were non-neoplastic and 76% (n=38) were neoplastic. There were an equal number of benign lesions in both sexes, while malignant lesions were more common in males compared to females, with a male to female ratio of 1.3:1. Out of the 12 (24%) non-neoplastic cases, 11 (21.6%) were cases of esophagitis, and one case was Barrett’s esophagus. A total of 38 (74.5%) cases were neoplastic. Among the neoplastic cases, all were malignant, with squamous cell carcinoma being the most common (Figure 2). Of the 11 cases of esophagitis, the maximum cases presented with erythematous changes on endoscopy. One case of Barrett’s esophagus presented as an ulcerative lesion. Ulceration with proliferative growth was commonly seen in squamous cell carcinomas, whereas ulceration was not commonly associated with adenocarcinoma. Adenocarcinoma presented as a proliferative lesion with or without ulceration.
The maximum biopsies from the stomach were obtained from the age group of 66-75 years, with a male to female ratio of 1.7:1. Out of the total 27 cases (n=18), benign lesions were more common, accounting for 66.7%, while 33.3% were malignant. Both benign and malignant lesions were more common in male patients. The most common benign lesion was gastritis (Figure 2), accounting for 48.1%, which peaked in the 66-75 years age group. Adenocarcinoma (Figure 2) was the most common malignant lesion, peaking in the 46-55 years age group.
Out of 13 cases of gastritis, nine cases presented as erythematous changes on endoscopy. The maximum cases (Six cases) of adenocarcinoma presented as an ulcer-proliferative growth on endoscopy, while hyperplastic polyps presented as polypoidal growths on endoscopy (Table 2).
The maximum biopsies of the duodenum were received from the 46-55 years age group, with a male to female ratio of 3.5:1. Out of 27 biopsies, the majority of the lesions were benign (25 cases, 92.6%), and two cases (7.4%) were neoplastic. Duodenitis (48%, 13/25) was the most common benign lesion encountered, followed by 33.3% of cases of celiac disease (Figure 2), hyperplastic polyp (7.4%), and a single case of tropical sprue. There were two cases of malignant duodenal lesions seen in elderly male patients (56-75 years). One patient had adenocarcinoma (Figure 2), and one had a well-differentiated neuroendocrine neoplasm.
|
d
|
|
a
|
Maximum cases of duodenitis (29.6%) presented as erythematous changes on endoscopy. Half of the cases of celiac disease presented as nodular growth, and half of the cases presented as atrophy or scalloping on endoscopy. Both cases of hyperplastic polyp presented as polypoidal growths on endoscopy (Table 3).
|
Table 1. Comparison of endoscopic findings with histopathology of non-neoplastic and neoplastic lesions of the esophagus and gastroesophageal junction
.PNG) Table 2. Comparison of endoscopic findings with histopathology findings of gastric lesions .PNG) Table 3. Comparison of endoscopic findings with histopathology findings of duodenal lesion .PNG) .PNG) Figure 2. Histomicrograph of upper GIT lesion, a: Stomach: Chronic Gastritis with Follicle Formation H & E X100, b: Duodenum: Adenocarcinoma Well-Differentiated H & E X 100 c: Stomach: Adenocarcinoma Well-Differentiated H & E X100, d: Signet Ring Adenocarcinoma H & E X10, e: Duodenum: Celiac Sprue with Villous Atrophy & Intra Epithelial Lymphocytes H & E X400, f: Esopghagus: Squamous Cell Carcinoma Moderately H & E X 100, Source: GCS medical college hospital and research center, Ahmedabad, Gujarat |
Discussion
Upper GI lesions are major causes of morbidity. Endoscopy visualizes and biopsies mucosal lesions, being minimally invasive and outpatient (4).
In the present study, the majority of the samples are from the esophagus, comprising 48.5%, followed by an equal number of cases from the stomach and duodenum, each comprising 25.7%. A study by Sharma et al. also showed that the majority of samples were from the esophagus, whereas other studies by Qureshi et al. (5), Vidyavathi et al. (6), Kothari et al. (7), Krishnappa et al. (8), Hussain et al. (2), and Abilash et al. (9) show that the majority of biopsies were from the stomach.
Demographic data related to age and sex in the present study show trends almost similar to those in other reported studies: Qureshi et al. (5), UK; Sacco et al. (10), USA; Vidyavathi et al. (6), India (Kolar); Krishnappa et al. (8), Bangalore; Hussain et al. (2), Kerala; and Abilash et al. (9), Srinagar, all showing male predominance. However, Choomsri et al. (11) reported female preponderance. The present study shows the highest number of upper GI endoscopic biopsies in the 5th and 6th decades of life, similar to other studies that also show a preponderance between 40-60 years of age. The reason for this finding is that males are comparatively more exposed to environmental pollutants than females and are more involved in habits such as smoking and tobacco consumption than females (12).
The present study shows a mild predominance of non-neoplastic lesions of the upper GI tract (52.4%), which is similar to other studies like Qureshi et al. (5) (17%), Krishnappa et al. (8) (44%), and Abilash et al. (9) (22%). However, other studies, such as those by Vidyavathi (6) and Hussain (2), show a predominance of neoplastic lesions.
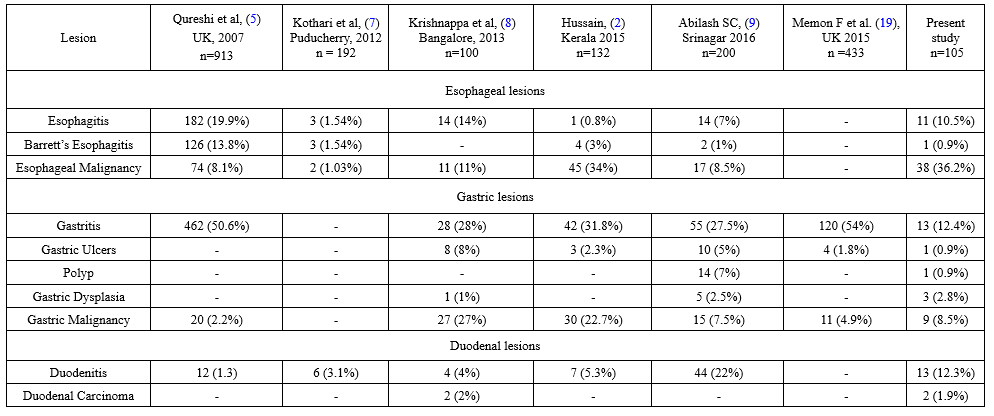
Chronic nonspecific oesophagitis (10.5%) was the most common diagnosis, similar to the studies by Qureshi et al. (5), Krishnappa et al. (8), and Abilash et al. (9). Abhilash et al. (9) and Kothari et al. (7) reported 1% and 1.5% of cases of Barrett’s esophagus, respectively. Ulceration is nearly always induced by gastroesophageal reflux and is reported to occur in 10% of patients with this condition. The main complications of Barrett’s esophagus include peptic ulcer, stricture, bleeding, and the development of dysplasia and adenocarcinoma (Table 4).
Dysplasia is found in Barrett’s esophagus in the absence of carcinoma in 5-10% of the cases and is associated with carcinoma in 68-100% of the cases. Malignant lesions were more common, accounting for 74.5% of the total esophageal biopsies (n=51), while 25.5% were non-neoplastic lesions. Similar findings were observed in studies conducted by Qureshi et al. (5) and Hussain et al. (2).
The American College of Gastroenterology recommends 1-year endoscopy for Barrett's mucosa, 6 months for low-grade dysplasia, and then yearly follow-ups. High-grade dysplasia patients require expert confirmation, repeat endoscopy within three months, and biopsies to exclude carcinoma from flat mucosa (2). Esophageal squamous dysplasia predicts esophageal squamous cell carcinoma. Found in ≥25% of adults above 35 years, it parallels carcinoma rates (13). Squamous cell carcinoma (71%) was the most common histological type in the malignant lesions, which is comparable to various studies (9,14,15) reporting rates ranging from 66% to 100%. In addition, 52.6% of patients with esophageal carcinoma were in the 56-75-year age group. These observations align with studies by Abhilash et al. (9) and Qureshi et al. (5). Esophageal cancer ranks eighth in incidence and sixth in mortality globally (16). Dawsey et al. (17) note that, in the West, adenocarcinoma is rising, while squamous cell carcinoma remains predominant elsewhere. Parkin et al. (16) state that 80% of esophageal carcinomas occur in developing countries, mostly esophageal squamous cell carcinoma. In India, it ranks as the third and fourth leading cancer in men and women, respectively (18).
In this study, overall inflammatory lesions were more prevalent in stomach biopsies, with chronic nonspecific gastritis being the most common diagnosis.
Memon et al. (19) and Gumber et al. (15) also showed similar trends. Gastritis with intestinal metaplasia or dysplasia is a significant histological finding, indicating a premalignant disease. In 11.1% of the cases, intestinal metaplasia/dysplasia was seen along with gastritis. A similar observation was also made by Abhilash et al. (9) and Krishnappa et al. (8). Only 8.5% of the gastric biopsies were diagnosed as malignancy on histology, adenocarcinoma being the histological type. Memon et al. (19) and Abhilash et al. (9) also reported a lower prevalence of malignancy, with frequencies of 5% and 7.5%, respectively.
Non-specific duodenitis was the most common lesion encountered in the duodenum. The duodenum has a rich, rapidly regenerating epithelial lining that can easily be affected by any inflammatory insult (19). The prevalence of inflammatory lesions in the duodenum was also demonstrated in studies by Abhilash et al. (9), Qureshi et al. (5), Hussain et al. (2), Krishnappa et al. (8), and Kothari et al. (7).
In this study, 33.3% of the cases had celiac disease. The Marsh-Oberhuber criteria, based on small bowel biopsies, are used for grading (20). Increased intraepithelial T lymphocytes suggest celiac disease even in the absence of villous atrophy (3). In this study, Type III (66.6%) was the most common, while Type I (11.1%) was the least common. In contrast, Memon (19) reported 76.1% of cases with suspected celiac disease, with mild cases being more prevalent. Difficulty in identifying intraepithelial T lymphocytes due to small biopsies may explain the lower number of Type I cases. Malignant cases in the duodenum were rare (1.9%), consistent with findings from other studies by Krishnappa et al. (8), Raychaudhuri et al. (21), and Khandige et al. (22).
Conclusion
This study highlights endoscopic patterns correlated with histopathology for early detection and treatment. It provides valuable insights into the demographic distribution, lesion types, and comparisons with other studies, aiding in understanding regional trends and advancing diagnostic approaches. Histopathology is crucial in assessing upper GI lesions from endoscopic biopsies, distinguishing between non-neoplastic, premalignant, and neoplastic conditions, especially in Barrett's esophagus. Esophageal biopsies were common, with malignancy in 47.6%, predominantly in the esophagus, particularly in those aged 50-60. Gastric and duodenal lesions are often benign, but suspicion and timely histopathological study aid early management. Accurate diagnosis improves patient outcomes while understanding lesion demographics aids in tailoring management. The synergy between endoscopy and histopathology enhances diagnostic precision, guiding optimal clinical decisions and improving care.
|
Table 4. Comparison of upper GI lesions with other studies
 |
Acknowledgement
The authors extend their sincere appreciation to the management and all staff in the Department of Pathology, Medical College and Research Center, Ahmedabad, Gujarat, where this study was conducted.
Funding sources
No funding sources.
Ethical statement
The study was approved by the Institutional Ethics Committee (GCSMC/EC/Dissertation/APPROVE/2019/0091).
Conflicts of interest
None declared.
Author contributions
All the authors have participated in one or more parts of the present study: Anupama Ishwar Dayal conducted the test; Tejas Atulbhai Contractor and Himali Parsotambhai Thakkar performed the data analysis and wrote the manuscript; Sandesh Omprakash Agrawal and Hani Kamleshbhai Patel collected the data.
Research Article: Research Article |
Subject:
Pathology
Received: 2024/06/6 | Accepted: 2024/12/7 | Published: 2025/04/26 | ePublished: 2025/04/26
Received: 2024/06/6 | Accepted: 2024/12/7 | Published: 2025/04/26 | ePublished: 2025/04/26
References
1. Jerold RT. The Gastrointestinal tract. In: Robbins and Cotran pathologic basis of disease. 10th ed. Philadelphia: Elsevier/Saunders. 2020; 753-822. [View at Publisher]
2. Hussain SI, Reshi R, Akhter G, Beigh A. Clinico histopathological study of upper gastrointestinal tract endoscopic biopsies. International Journal of Current Research and Review. 2015; 7(16): 78-85. [View at Publisher]
3. Goldblum JR, Lamps LW, McKenney JK, Myers JL, Ackerman LV, Rosai J, editors. Rosai and Ackerman's surgical pathology. Eleventh edition. Philadelphia, PA: Elsevier. 2018; 2 [View at Publisher] [Google Scholar]
4. Kaur S, Sharma R, Kaushal V, Gulati A, Sharma B. Diagnostic accuracy of endoscopic brush cytology in malignancies of upper gastrointestinal tract: A prospective study of 251 patients in North India. J Can Res Ther. 2016; 12(2): 681. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Qureshi NA, Hallissey MT, Fielding JW. Outcome of index upper gastrointestinal endoscopy in patients presenting with dysphagia in a tertiary care hospital-A 10 years review. BMC Gastroenterol. 2007; 7(1): 43. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Vidyavathi K, Harendrakumar M, Lakshmana Kumar Y. Correlation of endoscopic brush cytology with biopsy in diagnosis of upper gastrointestinal neoplasms. Indian J Pathol Microbiol. 2008; 51(4): 489. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Kothari SL, Dayal A, Patel SM. Interpretation of Upper Gastrointestinal Tract Mucosal Biopsies - A Tertiary Care Centre Experience. APALM. 2018; 5(8): A709-714. [View at Publisher] [DOI] [Google Scholar]
8. Krishnappa R, Horakerappa M, Ali K, Gouri M. A study on histopathological spectrum of upper gastrointestinal tract endoscopic biopsies. Inte Jour of Medi Res & Health Sci. 2013; 2(3): 418. [View at Publisher] [DOI]
9. Abilash, Kolakkadan H, Gitanjali, Shreelakshmidevi, Balamuruganvelu. Histopathologic Spectrum of Upper Gastrointestinal Tract Mucosal Biopsies : A Retrospective Study. In 2016. [View at Publisher]
10. Sacco F, Bruce MG, McMahon BJ, Bruden D. A prospective evaluation of 200 upper endoscopies performed in Alaska Native persons. International Journal of Circumpolar Health. 2007; 66(2): 144-52. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Choomsri P, Bumpenboon W, Wasuthit Y, Euanorasetr C, Sumritpradit P, Suwanthunma W, et al. Upper Gastrointestinal Endoscopy Findings in Patients Presenting with Dyspepsia. Thai J Surg. 2010; 31(1). [View at Publisher] [Google Scholar]
12. Parveen Malhotra PM, Kumar R, Chhabra S, Malhotra V, Sanwariya Y, Pahuja I. Brush cytology-alternative to endoscopic biopsy in diagnosing malignancy. GHOA. 2020; 11(3): 104-10. [DOI] [Google Scholar]
13. Taylor PR, Abnet CC, Dawsey SM. Squamous Dysplasia-The Precursor Lesion for Esophageal Squamous Cell Carcinoma. Cancer Epidemiology, Biomarkers & Prevention. 2013; 22(4): 540-52. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Aparajita A, Mohanty RC, Sahu AA, Mohanty R, Kumar P, Bhuyan T. Histomorphological Study of Upper GI Endoscopic Biopsies. International Journal of Health Sciences. 2016;(12). [View at Publisher]
15. Gumber R, Mulay SS. Endoscopic Biopsy Interpretation of Upper Gastrointestinal Pathologies. ijsr. 2016; 5(10): 20-4. [View at Publisher]
16. Parkin DM, Bray F, Ferlay J, Pisani P. Global Cancer Statistics, 2002. CA: A Cancer Journal for Clinicians. 2005; 55(2): 74-108. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Dawsey SP, Tonui S, Parker RK, Fitzwater JW, Dawsey SM, White RE, et al. Esophageal Cancer in Young People: A Case Series of 109 Cases and Review of the Literature. Ng IOL, editor. PLoS ONE. 2010; 5(11): e14080. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Khan N, Teli Ma, Mohib-ul Haq M, Bhat G, Lone MohdM, Afroz F. A survey of risk factors in carcinoma esophagus in the valley of Kashmir, Northern India. J Can Res Ther. 2011; 7(1): 15. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Memon DrF, Baloch DrK, Afzal Memon DrA. UPPER GASTROINTESTINAL ENDOSCOPIC BIOPSY; MORPHOLOGICAL SPECTRUM OF LESIONS. TPMJ. 2015; 22(12): 1574-9. [View at Publisher] [DOI] [Google Scholar]
20. Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. European Journal of Gastroenterology & Hepatology. 1999; 11(10): 1185. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Raychaudhuri S, Sharma N, Arora S, Pujani M, Rana D, Somani NS, et al. Comparative Study of Platelet Indices in Normal Pregnant and Non-Pregnant Women in a Tertiary Care Hospital in Northern India. APALM. 2018; 5(8): A683-688. [View at Publisher] [DOI] [Google Scholar]
22. Khandige S, Shetty S, Thapa R. The Conceding of Upper Gastrointestinal Lesion Endoscopic Biopsy: A Bare Minimum For Diagnosis. International Journal of Scientific Research. 2015; 4(2): 264-6. [View at Publisher]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.