
Thu, Sep 4, 2025




1- Department of Medical Laboratory Science, Faculty of Basic Medical Sciences, Osun State University, Osogbo, Osun State, Nigeria; Department of Medical Laboratory Science, Achievers University, Owo, Ondo State, Nigeria , adedeji.atere@uniosun.edu.ng
2- Department of Medical Laboratory Science, Achievers University, Owo, Ondo State, Nigeria
3- Department of Medical Laboratory Science, Faculty of Basic Medical Sciences, Osun State University, Osogbo, Osun State, Nigeria
2- Department of Medical Laboratory Science, Achievers University, Owo, Ondo State, Nigeria
3- Department of Medical Laboratory Science, Faculty of Basic Medical Sciences, Osun State University, Osogbo, Osun State, Nigeria
Full-Text [PDF 397 kb]
(226 Downloads)
| Abstract (HTML) (828 Views)
Discussion
The findings of this study shed light on the intricate relationship between menopausal status, bone-associated biomarkers, and PTH levels in postmenopausal women. Understanding these associations is crucial for elucidating osteoporosis risk factors and implementing effective strategies for bone health maintenance in this vulnerable population. Anthropometric characteristics, including BMI and blood pressure, are significant determinants of overall health status and are often influenced by hormonal changes associated with menopause. Consistent with previous research (18,19), our study revealed a notable increase in BMI among postmenopausal women compared to premenopausal and reproductive-age counterparts. The rise in obesity rates may be attributed to menopause-induced alterations in adiposity and fat distribution, emphasizing the importance of targeted interventions to mitigate obesity-related health risks in postmenopausal women.
The comparative analysis of bone-associated biomarkers across reproductive life stages revealed noteworthy variations in serum levels, underscoring the impact of hormonal fluctuations on bone metabolism. Postmenopausal women exhibited significantly lower serum calcium and estradiol levels compared to premenopausal and reproductive-age groups, consistent with prior findings (20-22). The decline in calcium and estradiol levels indicates the increased risk of bone mineral density loss and osteoporosis in postmenopausal women, necessitating proactive measures such as calcium supplementation and hormone replacement therapy to mitigate bone health deterioration.
Interestingly, postmenopausal women demonstrated elevated plasma phosphorus and alkaline phosphatase levels compared to their younger counterparts. These findings are in line with existing literature (23) and suggest increased bone turnover and remodeling processes characteristic of osteoporosis. Moreover, the significant positive correlation between PTH and calcium, vitamin D, and estradiol levels in postmenopausal women highlights the regulatory role of PTH in calcium homeostasis and bone metabolism, corroborating previous research findings (19,24).
The observed association between menopausal status and plasma vitamin D levels highlights the heightened risk of vitamin D deficiency among postmenopausal women, predisposing them to impaired calcium absorption and compromised bone health. Consistent with previous studies (11,25), our findings highlight the relevance of vitamin D supplementation in maintaining optimal bone mineral density and reducing osteoporosis risk in postmenopausal women.
In the study, the reproductive age group exhibited significantly higher levels of biomarkers, including ALP, uric acid, calcium, PTH, vitamin D, and estradiol, compared to the post-menopausal group (p <0.001). Blood uric acid (sUA) may play a beneficial role in bone metabolism due to its antioxidant properties in postmenopausal women. Osteoporosis development is closely linked to oxidative stress, and sUA, being the end product of purine metabolism, possesses extracellular antioxidant properties that are believed to protect bone metabolism (26,27). This relationship explains why uric acid levels are lower in post-menopausal women.
However, the study has some limitations, such as a small sample size of participants, which restricts the generalizability of the findings. Longitudinal biomarker data and ethnic, regional, and demographic variability investigations are also lacking. To overcome these constraints, future studies that focus on longitudinal biomarker trends over time should be conducted. Generalizability can be improved by including larger, more diverse populations in the research. It would also be beneficial to explore how factors like lifestyle interventions, genetics, and comorbidities influence the risk of osteoporosis in postmenopausal women to gain a more comprehensive understanding of bone health.
Conclusion
This study provides valuable insights into the complex interplay between menopausal status, bone-associated biomarkers, and PTH levels in postmenopausal women. Our findings highlight the increased risk of osteoporosis and bone health deterioration in postmenopausal women, characterized by dysregulated plasma levels of calcium, vitamin D, estradiol, phosphorus, alkaline phosphatase, and uric acid. The observed correlations between PTH and various bone-associated biomarkers highlight the pivotal role of PTH in modulating bone metabolism and calcium homeostasis.
Acknowledgement
The authors thank all participants and medical staff of the Gynecology and Obstetrics clinic at the FMC, Owo, for their support.
Funding sources
Nil.
Ethical statement
Informed consent was obtained from all participants, and the Ethics Committee of the Federal Medical Center, Owo (Reference number FMC/OW/380/VOL.CL/184) approved the study.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Author contributions
ADA and EEE designed the study and drafted the first manuscript. KYA and IIP designed and reviewed the final manuscript for intellectual content. All authors contributed to the final version of the manuscript and are responsible for the integrity and accuracy of this review.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Full-Text: (25 Views)
Introduction
Menopause, a natural phenomenon marking the cessation of menstrual periods in women, signifies a pivotal hormonal transition often associated with various health implications, notably bone diseases. It occurs typically between the ages of 48 and 52 years and is characterized by declining levels of estrogen and progesterone due to decreased ovarian function (1). Postmenopausal status, defined as the absence of menstruation for at least 12 consecutive months, represents a significant physiological shift, particularly impacting bone metabolism and calcium homeostasis (2,3). The pathophysiology is mostly due to an imbalance in bone turnover caused by a decrease in estrogen secretion. Ovarian function and estrogen levels decline in postmenopausal women, leading to decreased bone production and increased bone resorption during bone remodeling, which lowers bone mass, density, and fracture risk. Osteoporosis results from a number of factors, including hormonal changes and calcium and vitamin D insufficiency, and there is growing evidence that oxidative stress may also contribute to age-related bone loss by boosting osteoclast bone resorption (4-6).
Parathyroid hormone (PTH), a crucial regulator of serum calcium levels, plays a central role in bone remodeling by influencing osteoclast activity and bone turnover (7,8). Imbalances in PTH secretion, such as hypo parathyroidism- or hyperparathyroidism, can disrupt calcium metabolism and contribute to bone diseases like osteoporosis (9). Additionally, vitamin D deficiency, often prevalent in postmenopausal women, further exacerbates bone health issues by impairing calcium absorption and mineralization (10,11).
Bone-associated biomarkers, including alkaline phosphatase (ALP), inorganic phosphate, and uric acid, serve as indicators of bone turnover and remodeling processes. Dysregulation of these markers can signify abnormalities in bone metabolism and potential osteoporotic risk (12-14). Despite advancements in understanding bone metabolism and the role of hormonal changes in menopause, there remains a gap in comprehensively elucidating the interplay between postmenopausal status, bone-associated biomarkers, and PTH levels.
Therefore, this study aimed to investigate the correlative relationship between bone-associated biomarkers and PTH levels in postmenopausal women in Owo metropolis. By measuring the levels of PTH, vitamin D, uric acid, calcium, phosphorus, ALP, and estradiol, we aimed to provide insights into the bone health status of postmenopausal women and the potential implications for osteoporosis risk assessment.
Methods
Experimental design
This cross-sectional study was conducted from January to July. A total of sixty postmenopausal subjects aged 48 to 60 were recruited for the study. Postmenopausal status was defined as the absence of menstrual flow for a minimum of 12 consecutive months, assuming participants had a uterus and were not pregnant or lactating (2). Additionally, twenty premenopausal women and twenty reproductive-age women, aged 30 to 50 years, were included as control groups. Comprehensive medical histories and personal data were collected using a structured questionnaire following approval from the Ethics Committee of the Federal Medical Center, Owo (Ethics number: FMC/OW/380/VOL.CL/184). Informed consent was obtained from all participants.
Sample size determination
The sample size for this study was arrived at using the formula n = Z²p (1 - p)/d² as propounded by Daniel (15). According to Adewale et al., a prevalence of 3.5% for hip osteoarthritis in Black Nigerian women of ages 50 years and above was determined (16). In the formula, “n” represents the minimum sample size required; “Z” is the standard normal deviate set at 1.96 corresponding to the 95% confidence level; and “d” is the absolute precision level set as 5% or 0.05. Hence, the minimum sample size required was estimated at 52; nevertheless, 60 respondents were purposively selected to provide for missing data or non-responses in the study.
Inclusion and exclusion criteria
Inclusion criteria for postmenopausal women included informed consent and age between 48 to 60 years. Premenopausal and reproductive-age women were included as controls based on similar inclusion criteria. Exclusion criteria comprised subjects younger than 30 years, the presence of serious or unstable medical disorders, and immunocompromised individuals.
Samples collection and storage
Blood samples were taken from each participant using standard protocols. 5 milliliters (5ml) of venous blood were drawn into sterile lithium heparin bottles. After gentle mixing, the samples were centrifuged at 4000 revolutions per minute (rpm) for 5 minutes to extract serum. Serum was kept at -20 °C until it was analyzed for PTH, vitamin D, uric acid, calcium, phosphorus, and alkaline phosphatase levels.
Analytical methods
Using reagents provided by Randox Laboratories Ltd. (UK), standard enzymatic methods were used to determine plasma levels of ALP, phosphorus, uric acid, and calcium. An ELISA kit from Melsin Medical Company, USA, was used to assess the serum levels of vitamin D, PTH and estradiol. Every participant had their height and weight measured, and their body mass index (BMI) was calculated using the guidelines provided by Atere et al. (17).
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.0 0 (SPSS Inc., Chicago, IL, USA). Normality was assessed using the Shapiro-Wilk test, and homogeneity of variances with Levene’s test. One-way ANOVA was used for comparing group means; non-parametric alternatives were applied where assumptions were violated. Spearman’s correlation coefficients were used to assess relationships between PTH and bone-associated biomarkers based on data distribution. Receiver operating characteristic (ROC) analysis determined the diagnostic accuracy of biomarkers. Results were reported as mean ± standard deviation (SD), with a significant level of 0.05 (p = 0.05) considered statistically significant.
Results
Anthropometric characteristics were assessed across three distinct groups: pre-menopausal, reproductive-aged, and post-menopausal women, with the former two serving as controls for the latter experimental group. ANOVA results indicated statistically significant differences in age and systolic blood pressure among the groups (p <0.001). However, there were no notable statistical differences in body mass index (BMI) and diastolic blood pressure (Figure 1).
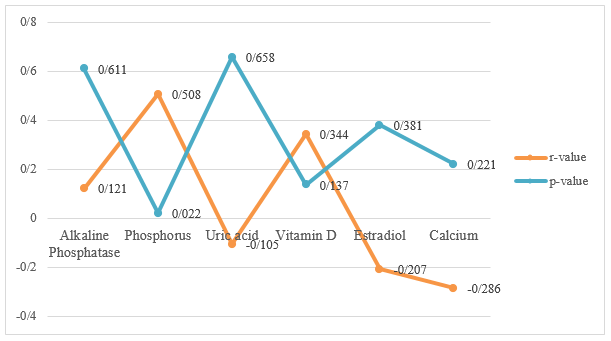
Table 1 compares the bone-associated biomarkers of the groups. The reproductive age group had considerably greater levels of biomarkers, including ALP, uric acid, calcium, PTH, vitamin D, and estradiol, while the post-menopausal group had lower levels (p <0.001). Figure 2 displays the connection of biomarkers with PTH in postmenopausal women. It was observed that ALP and phosphorus had a significant negative correlation with PTH, while calcium, vitamin D, and estradiol showed a significant positive correlation with PTH. Figure 3 illustrates how biomarkers correlate with PTH in premenopausal women. Only phosphorus had a significant positive correlation with PTH (p <0.05), while uric acid, estradiol, and calcium had a statistically insignificant negative link with PTH.
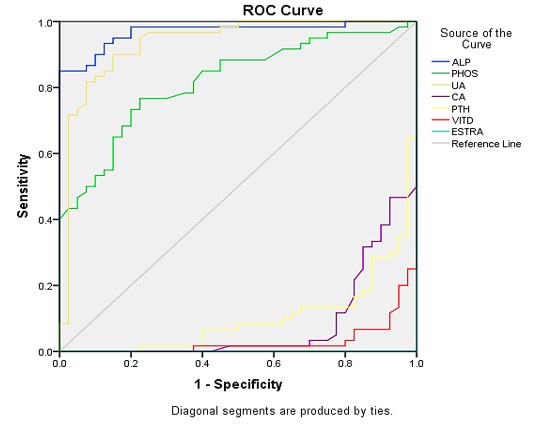
Figure 4 depicts the ROC curve for the sensitivity and specificity of the PTH and bone-associated biomarkers. Alkaline phosphatase, phosphorus, and uric acid all have good sensitivity and specificity, as evidenced by their ROC curves. Calcium, PTH, and vitamin D have lower sensitivity and specificity as evidenced by their ROC curves, but estradiol has no suggested specificity or sensitivity as indicated by the absence of a curve line and an area under curve (AUC) value of zero.
Menopause, a natural phenomenon marking the cessation of menstrual periods in women, signifies a pivotal hormonal transition often associated with various health implications, notably bone diseases. It occurs typically between the ages of 48 and 52 years and is characterized by declining levels of estrogen and progesterone due to decreased ovarian function (1). Postmenopausal status, defined as the absence of menstruation for at least 12 consecutive months, represents a significant physiological shift, particularly impacting bone metabolism and calcium homeostasis (2,3). The pathophysiology is mostly due to an imbalance in bone turnover caused by a decrease in estrogen secretion. Ovarian function and estrogen levels decline in postmenopausal women, leading to decreased bone production and increased bone resorption during bone remodeling, which lowers bone mass, density, and fracture risk. Osteoporosis results from a number of factors, including hormonal changes and calcium and vitamin D insufficiency, and there is growing evidence that oxidative stress may also contribute to age-related bone loss by boosting osteoclast bone resorption (4-6).
Parathyroid hormone (PTH), a crucial regulator of serum calcium levels, plays a central role in bone remodeling by influencing osteoclast activity and bone turnover (7,8). Imbalances in PTH secretion, such as hypo parathyroidism- or hyperparathyroidism, can disrupt calcium metabolism and contribute to bone diseases like osteoporosis (9). Additionally, vitamin D deficiency, often prevalent in postmenopausal women, further exacerbates bone health issues by impairing calcium absorption and mineralization (10,11).
Bone-associated biomarkers, including alkaline phosphatase (ALP), inorganic phosphate, and uric acid, serve as indicators of bone turnover and remodeling processes. Dysregulation of these markers can signify abnormalities in bone metabolism and potential osteoporotic risk (12-14). Despite advancements in understanding bone metabolism and the role of hormonal changes in menopause, there remains a gap in comprehensively elucidating the interplay between postmenopausal status, bone-associated biomarkers, and PTH levels.
Therefore, this study aimed to investigate the correlative relationship between bone-associated biomarkers and PTH levels in postmenopausal women in Owo metropolis. By measuring the levels of PTH, vitamin D, uric acid, calcium, phosphorus, ALP, and estradiol, we aimed to provide insights into the bone health status of postmenopausal women and the potential implications for osteoporosis risk assessment.
Methods
Experimental design
This cross-sectional study was conducted from January to July. A total of sixty postmenopausal subjects aged 48 to 60 were recruited for the study. Postmenopausal status was defined as the absence of menstrual flow for a minimum of 12 consecutive months, assuming participants had a uterus and were not pregnant or lactating (2). Additionally, twenty premenopausal women and twenty reproductive-age women, aged 30 to 50 years, were included as control groups. Comprehensive medical histories and personal data were collected using a structured questionnaire following approval from the Ethics Committee of the Federal Medical Center, Owo (Ethics number: FMC/OW/380/VOL.CL/184). Informed consent was obtained from all participants.
Sample size determination
The sample size for this study was arrived at using the formula n = Z²p (1 - p)/d² as propounded by Daniel (15). According to Adewale et al., a prevalence of 3.5% for hip osteoarthritis in Black Nigerian women of ages 50 years and above was determined (16). In the formula, “n” represents the minimum sample size required; “Z” is the standard normal deviate set at 1.96 corresponding to the 95% confidence level; and “d” is the absolute precision level set as 5% or 0.05. Hence, the minimum sample size required was estimated at 52; nevertheless, 60 respondents were purposively selected to provide for missing data or non-responses in the study.
Inclusion and exclusion criteria
Inclusion criteria for postmenopausal women included informed consent and age between 48 to 60 years. Premenopausal and reproductive-age women were included as controls based on similar inclusion criteria. Exclusion criteria comprised subjects younger than 30 years, the presence of serious or unstable medical disorders, and immunocompromised individuals.
Samples collection and storage
Blood samples were taken from each participant using standard protocols. 5 milliliters (5ml) of venous blood were drawn into sterile lithium heparin bottles. After gentle mixing, the samples were centrifuged at 4000 revolutions per minute (rpm) for 5 minutes to extract serum. Serum was kept at -20 °C until it was analyzed for PTH, vitamin D, uric acid, calcium, phosphorus, and alkaline phosphatase levels.
Analytical methods
Using reagents provided by Randox Laboratories Ltd. (UK), standard enzymatic methods were used to determine plasma levels of ALP, phosphorus, uric acid, and calcium. An ELISA kit from Melsin Medical Company, USA, was used to assess the serum levels of vitamin D, PTH and estradiol. Every participant had their height and weight measured, and their body mass index (BMI) was calculated using the guidelines provided by Atere et al. (17).
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.0 0 (SPSS Inc., Chicago, IL, USA). Normality was assessed using the Shapiro-Wilk test, and homogeneity of variances with Levene’s test. One-way ANOVA was used for comparing group means; non-parametric alternatives were applied where assumptions were violated. Spearman’s correlation coefficients were used to assess relationships between PTH and bone-associated biomarkers based on data distribution. Receiver operating characteristic (ROC) analysis determined the diagnostic accuracy of biomarkers. Results were reported as mean ± standard deviation (SD), with a significant level of 0.05 (p = 0.05) considered statistically significant.
Results
Anthropometric characteristics were assessed across three distinct groups: pre-menopausal, reproductive-aged, and post-menopausal women, with the former two serving as controls for the latter experimental group. ANOVA results indicated statistically significant differences in age and systolic blood pressure among the groups (p <0.001). However, there were no notable statistical differences in body mass index (BMI) and diastolic blood pressure (Figure 1).
Table 1 compares the bone-associated biomarkers of the groups. The reproductive age group had considerably greater levels of biomarkers, including ALP, uric acid, calcium, PTH, vitamin D, and estradiol, while the post-menopausal group had lower levels (p <0.001). Figure 2 displays the connection of biomarkers with PTH in postmenopausal women. It was observed that ALP and phosphorus had a significant negative correlation with PTH, while calcium, vitamin D, and estradiol showed a significant positive correlation with PTH. Figure 3 illustrates how biomarkers correlate with PTH in premenopausal women. Only phosphorus had a significant positive correlation with PTH (p <0.05), while uric acid, estradiol, and calcium had a statistically insignificant negative link with PTH.
Figure 4 depicts the ROC curve for the sensitivity and specificity of the PTH and bone-associated biomarkers. Alkaline phosphatase, phosphorus, and uric acid all have good sensitivity and specificity, as evidenced by their ROC curves. Calcium, PTH, and vitamin D have lower sensitivity and specificity as evidenced by their ROC curves, but estradiol has no suggested specificity or sensitivity as indicated by the absence of a curve line and an area under curve (AUC) value of zero.
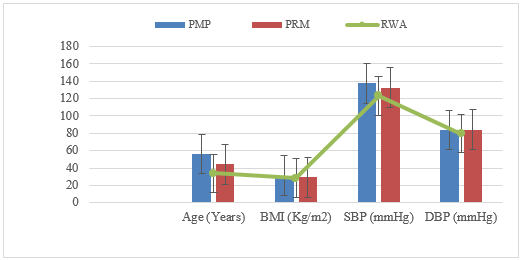 Figure 1. Anthropometric Characteristics of the Recruited Subjects Key: BMI = Body Mass Index, SBP = Systolic Blood Pressure, DBP = Diastolic Blood Pressure, PMP = Postmenopausal women, PRM = Premenopausal women; RWA = Reproductive Women Age Table 1. Comparison of bone-related biomarkers among post-menopausal, pre-menopausal, and reproductive age women 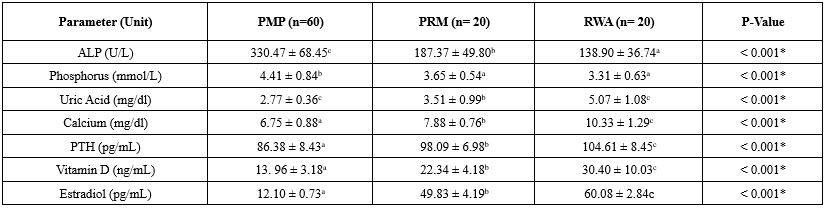 * Significant level=0.05 a = postmenopausal women; b = premenopausal women; c = reproductive age women *Values were represented with Mean±SD. Mean values were compared using one-way ANOVA with a level of significance of 0.05. Values in the same column with the same superscript are not statistically different at p <0.05 using the post-Hoc test. Key: n=sample size, ALP = Alkaline Phosphatase, PTH = Parathyroid Hormone, PMP = Postmenopausal women, PRM = Premenopausal women; RWA = Reproductive Women Age |

Discussion
The findings of this study shed light on the intricate relationship between menopausal status, bone-associated biomarkers, and PTH levels in postmenopausal women. Understanding these associations is crucial for elucidating osteoporosis risk factors and implementing effective strategies for bone health maintenance in this vulnerable population. Anthropometric characteristics, including BMI and blood pressure, are significant determinants of overall health status and are often influenced by hormonal changes associated with menopause. Consistent with previous research (18,19), our study revealed a notable increase in BMI among postmenopausal women compared to premenopausal and reproductive-age counterparts. The rise in obesity rates may be attributed to menopause-induced alterations in adiposity and fat distribution, emphasizing the importance of targeted interventions to mitigate obesity-related health risks in postmenopausal women.
The comparative analysis of bone-associated biomarkers across reproductive life stages revealed noteworthy variations in serum levels, underscoring the impact of hormonal fluctuations on bone metabolism. Postmenopausal women exhibited significantly lower serum calcium and estradiol levels compared to premenopausal and reproductive-age groups, consistent with prior findings (20-22). The decline in calcium and estradiol levels indicates the increased risk of bone mineral density loss and osteoporosis in postmenopausal women, necessitating proactive measures such as calcium supplementation and hormone replacement therapy to mitigate bone health deterioration.
Interestingly, postmenopausal women demonstrated elevated plasma phosphorus and alkaline phosphatase levels compared to their younger counterparts. These findings are in line with existing literature (23) and suggest increased bone turnover and remodeling processes characteristic of osteoporosis. Moreover, the significant positive correlation between PTH and calcium, vitamin D, and estradiol levels in postmenopausal women highlights the regulatory role of PTH in calcium homeostasis and bone metabolism, corroborating previous research findings (19,24).
The observed association between menopausal status and plasma vitamin D levels highlights the heightened risk of vitamin D deficiency among postmenopausal women, predisposing them to impaired calcium absorption and compromised bone health. Consistent with previous studies (11,25), our findings highlight the relevance of vitamin D supplementation in maintaining optimal bone mineral density and reducing osteoporosis risk in postmenopausal women.
In the study, the reproductive age group exhibited significantly higher levels of biomarkers, including ALP, uric acid, calcium, PTH, vitamin D, and estradiol, compared to the post-menopausal group (p <0.001). Blood uric acid (sUA) may play a beneficial role in bone metabolism due to its antioxidant properties in postmenopausal women. Osteoporosis development is closely linked to oxidative stress, and sUA, being the end product of purine metabolism, possesses extracellular antioxidant properties that are believed to protect bone metabolism (26,27). This relationship explains why uric acid levels are lower in post-menopausal women.
However, the study has some limitations, such as a small sample size of participants, which restricts the generalizability of the findings. Longitudinal biomarker data and ethnic, regional, and demographic variability investigations are also lacking. To overcome these constraints, future studies that focus on longitudinal biomarker trends over time should be conducted. Generalizability can be improved by including larger, more diverse populations in the research. It would also be beneficial to explore how factors like lifestyle interventions, genetics, and comorbidities influence the risk of osteoporosis in postmenopausal women to gain a more comprehensive understanding of bone health.
Conclusion
This study provides valuable insights into the complex interplay between menopausal status, bone-associated biomarkers, and PTH levels in postmenopausal women. Our findings highlight the increased risk of osteoporosis and bone health deterioration in postmenopausal women, characterized by dysregulated plasma levels of calcium, vitamin D, estradiol, phosphorus, alkaline phosphatase, and uric acid. The observed correlations between PTH and various bone-associated biomarkers highlight the pivotal role of PTH in modulating bone metabolism and calcium homeostasis.
Acknowledgement
The authors thank all participants and medical staff of the Gynecology and Obstetrics clinic at the FMC, Owo, for their support.
Funding sources
Nil.
Ethical statement
Informed consent was obtained from all participants, and the Ethics Committee of the Federal Medical Center, Owo (Reference number FMC/OW/380/VOL.CL/184) approved the study.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Author contributions
ADA and EEE designed the study and drafted the first manuscript. KYA and IIP designed and reviewed the final manuscript for intellectual content. All authors contributed to the final version of the manuscript and are responsible for the integrity and accuracy of this review.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Research Article: Research Article |
Subject:
Laboratory Sciences
Received: 2024/06/24 | Accepted: 2024/11/11
Received: 2024/06/24 | Accepted: 2024/11/11
References
1. Takahashi TA, Johnson KM. Menopause. Med Clin North Am. 2015;99(3):521-34. [View at Publisher] [DOI] [PMID]
2. Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Fertil Steril. 2012;94(4):843-51. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Scally NP, Armstrong L, Blades D, McGeown E, Mathers H. Menopausal Symptoms and Utian Quality of Life Scale Following a Breast Cancer Diagnosis and Its Impact on Endocrine Adherence. Cureus. 2024;16(1):e52777. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Effendy NM, Shuid AN. Time and dose-dependent effects of Labisia pumila on bone oxidative status of postmenopausal osteoporosis rat model. Nutrients. 2014;6(8):3288-302. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Park JM, Lee YJ. Serum oestradiol levels are inversely associated with C-reactive protein levels in premenopausal women, but not postmenopausal women. J Int Med Res. 2020;48(10):300060520961228. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Anklam CFV, Lissarassa YPS, Dos Santos AB, Costa-Beber LC, Sulzbacher LM, Goettems-Fiorin PB, et al. Oxidative and Cellular Stress Markers in Postmenopause Women with Diabetes: The Impact of Years of Menopause. J Diabetes Res. 2021;2021:3314871. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Tuchendler D, Bolanowski M. Assessment of bone metabolism in premenopausal females with hyperthyroidism and hypothyroidism. Endokrynol Pol. 2013;64(1):40-4. [View at Publisher] [PMID] [Google Scholar]
8. Kužma M, Jackuliak P, Killinger Z, Payer J. Parathyroid Hormone-Related Changes of Bone Structure. Physiol Res. 2021;70:3-11. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Bolland MJ, Grey A, Gamble GD, Reid IR. Calcium and vitamin D supplements and health outcomes: A reanalysis of the Women's Health Initiative (WHI) limited-access data set. Am J Clin Nutr. 2011;94(4):1144-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Holick MF. Vitamin D: a d-lightful solution for health. J Investig Med. 2011;59(6):872-80. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Khan AW, Zadran N, Khan A, Ishaq M, Kumar J, Ibrar A, et al. Vitamin D Levels and Bone Mineral Density in Premenopausal Women Compared to Postmenopausal Women: A Multi-Centre Study from Pakistan. Cureus. 2020;12(11):e11439. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Rosen CJ, Bilezikian JP. Clinical review 123: Hot topic - Anabolic therapy for osteoporosis. J Clin Endocrinol Metab. 2001;86(3):957-64. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12(20 Pt 2):6243s-9s. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Milic J, Renzetti S, Morini D, Motta F, Carli F, Menozzi M, et al. Bone Mineral Density and Trabecular Bone Score Changes throughout Menopause in Women with HIV. Viruses. 2023;15(12):2375. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Daniel WW, Crross CL. BIOSTATISTICS. A Foundation For Analysis In The Health Sciences. 2013. [View at Publisher] [Google Scholar]
16. Adewole OA, Idowu SO, Shoga MO, Kayode MO, Adelowo OO. Frequency of Osteoporosis in Black Nigerian Women Aged 50 and above with Degenerative Musculoskeletal Diseases and Fractures. West Afr J Med. 2021;38(4):342-6. [View at Publisher] [PMID] [Google Scholar]
17. Atere AD, Moronkeji A, Moronkeji AI, Osadolor HB. Serum levels of inflammatory biomarkers, glycaemic control indices and leptin receptors expression in adult male Wistar rats exposed to Pyrethroids. J Cell Biotechnol. 2021;7(1):41-55. [View at Publisher] [DOI] [Google Scholar]
18. Zanchetti A, Facchetti R, Cesana GC, Modena MG, Pirrelli A, Sega R, et al. Menopause-related blood pressure increase and its relationship to age and body mass index: The SIMONA epidemiological study. J Hypertens. 2005;23(12):2269-76. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Achie LN, Olorunshola K V, Igashi J, Toryila JE. Assessment of the levels of serum parathyroid hormone in rural postmenopausal women in Zuturung district, Zangon Kataf Local Government Area, Kaduna State, Nigeria. J Afr Assoc Physiol Sci. 2021;9(2):130-7. [View at Publisher] [Google Scholar]
20. Tuomisto H, Salo P, Saarinen R, Kalleinen N, Polo-Kantola P. The association of serum oestradiol level, age, and education with cognitive performance in peri- and late postmenopausal women. Maturitas. 2012;71(2):173-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Cano A, Chedraui P, Goulis DG, Lopes P, Mishra G, Mueck A, et al. Calcium in the prevention of postmenopausal osteoporosis: EMAS clinical guide. Maturitas. 2018;107:7-12. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Pardhe BD, Pathak S, Bhetwal A, Ghimire S, Shakya S, Khanal PR, et al. Effect of age and estrogen on biochemical markers of bone turnover in postmenopausal women: a population-based study from Nepal. Int J Womens Health. 2017;9:781-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Oluboyo AO, Anaenye C V, Oluboyo BO, Ajayi FO. Assessment of the Levels of Parathyroid Hormone, Oestrogen and Selected Bone Minerals in Menopausal Women. Am J Biomed Sci. 2018;10(4):189-194. [View at Publisher] [DOI] [Google Scholar]
24. Shi JW, Wu JN, Zhu XY, Zhou WH, Yang JY, Li MQ. Association of serum 25-hydroxyvitamin D levels with all-cause and cause-specific mortality among postmenopausal females: results from NHANES. J Transl Med. 2023;21(1):1-11. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Raju A, Luthra G, Shahbaz M, Almatooq H, Foucambert P, Esbrand FD, et al. Role of Vitamin D Deficiency in Increased Susceptibility to Respiratory Infections Among Children: A Systematic Review. Cureus. 2022;14(9):e29205. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Hak AE, Choi HK. Menopause, postmenopausal hormone use and serum uric acid levels in US women - The Third National Health and Nutrition Examination Survey. Arthritis Res Ther. 2008;10(5):1-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Sautin YY, Johnson RJ. Uric acid: the oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids. 2008;27(6):608-19. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Enamad


This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.